
In this chapter, we will clarify what psychological disorders are, how they are diagnosed and classified, their symptoms, and insights into their causes. There are many myths surrounding mental illness, so let’s begin by addressing a few of them.
Mental Health Myths
Myth: Mental health problems don’t affect me.
Fact: Mental health problems are actually very common. In 2014, about:
- One in five American adults experienced a mental health issue
- One in 10 young people experienced a period of major depression
- One in 25 Americans lived with a serious mental illness, such as schizophrenia, bipolar disorder, or major depression
Suicide is the 10th leading cause of death in the United States. It accounts for the loss of more than 41,000 American lives each year, more than double the number of lives lost to homicide. Learn more about mental health problems.
Myth: Children don’t experience mental health problems.
Fact: Even very young children may show early warning signs of mental health concerns. These mental health problems are often clinically diagnosable, and can be a product of the interaction of biological, psychological, and social factors.
Half of all mental health disorders show first signs before a person turns 14 years old, and three-quarters of mental health disorders begin before age 24.
Unfortunately, less than 20% of children and adolescents with diagnosable mental health problems receive the treatment they need. Early mental health support can help a child before problems interfere with other developmental needs.
Myth: People with mental health problems are violent and unpredictable.
Fact: The vast majority of people with mental health problems are no more likely to be violent than anyone else. Most people with mental illness are not violent and only 3%–5% of violent acts can be attributed to individuals living with a serious mental illness. In fact, people with severe mental illnesses are over 10 times more likely to be victims of violent crime than the general population. You probably know someone with a mental health problem and don’t even realize it, because many people with mental health problems are highly active and productive members of our communities.
Myth: People with mental health needs, even those who are managing their mental illness, cannot tolerate the stress of holding down a job.
Fact: People with mental health problems are just as productive as other employees. Employers who hire people with mental health problems report good attendance and punctuality as well as motivation, good work, and job tenure on par with or greater than other employees.
When employees with mental health problems receive effective treatment, it can result in:
- Lower total medical costs
- Increased productivity
- Lower absenteeism
- Decreased disability costs
Myth: Personality weakness or character flaws cause mental health problems. People with mental health problems can snap out of it if they try hard enough.
Fact: Mental health problems have nothing to do with being lazy or weak and many people need help to get better. Many factors contribute to mental health problems, including:
- Biological factors, such as genes, physical illness, injury, or brain chemistry
- Life experiences, such as trauma or a history of abuse
- Family history of mental health problems
People with mental health problems can get better and many recover completely. Learn more about mental health recovery here.
Myth: There is no hope for people with mental health problems. Once a friend or family member develops mental health problems, he or she will never recover.
Fact: Studies show that people with mental health problems get better and many recover completely. Recovery refers to the process in which people are able to live, work, learn, and participate fully in their communities. There are more treatments, services, and community support systems than ever before, and they work.
Myth: Therapy and self-help are a waste of time. Why bother when you can just take a pill?
Fact: Treatment for mental health problems varies depending on the individual and could include medication, therapy, or both. Many individuals work with a support system during the healing and recovery process.
Myth: I can’t do anything for a person with a mental health problem.
Fact: Friends and loved ones can make a big difference. Only 44% of adults with diagnosable mental health problems and less than 20% of children and adolescents receive needed treatment. Friends and family can be important influences to help someone get the treatment and services they need by:
- Reaching out and letting them know you are available to help
- Helping them access mental health services
- Learning and sharing the facts about mental health, especially if you hear something that isn’t true
- Treating them with respect, just as you would anyone else
- Refusing to define them by their diagnosis or using labels such as “crazy”
Myth: Prevention doesn’t work. It is impossible to prevent mental illnesses.
Fact: Prevention of mental, emotional, and behavioral disorders focuses on addressing known risk factors such as exposure to trauma that can affect the chances that children, youth, and young adults will develop mental health problems. Promoting the social-emotional well-being of children and youth leads to:
- Higher overall productivity
- Better educational outcomes
- Lower crime rates
- Stronger economies
- Lower health care costs
- Improved quality of life
- Increased lifespan
- Improved family lifeWhat you’ll learn to do: define psychological disorders and explain how they are classified
Psychological Disorders
 Psychological disorders are conditions characterized by abnormal thoughts, feelings, and behaviors. Although challenging, it is essential for psychologists and mental health professionals to agree on what experiences and actions constitute the presence of a psychological disorder. Inner experiences and behaviors that are atypical or violate social norms could signify the presence of a disorder; however, each of these criteria alone is inadequate. It is generally accepted that a psychological disorder is defined by significant disturbances in thoughts, feelings, and behaviors; these disturbances must reflect some kind of dysfunction (biological, psychological, or developmental), must cause significant impairment in one’s life, and must not reflect culturally expected reactions to certain life events.
Psychological disorders are conditions characterized by abnormal thoughts, feelings, and behaviors. Although challenging, it is essential for psychologists and mental health professionals to agree on what experiences and actions constitute the presence of a psychological disorder. Inner experiences and behaviors that are atypical or violate social norms could signify the presence of a disorder; however, each of these criteria alone is inadequate. It is generally accepted that a psychological disorder is defined by significant disturbances in thoughts, feelings, and behaviors; these disturbances must reflect some kind of dysfunction (biological, psychological, or developmental), must cause significant impairment in one’s life, and must not reflect culturally expected reactions to certain life events.
In this section, you’ll learn about how disorders are defined, and also how they are diagnosed and classified. The Diagnostic and Statistical Manual of Mental Disorders (DSM-5) is essentially a classification manual that clinicians can use to read about the criteria, prevalence, risk factors, and details about over 200 disorders.
Psychological Disorders
Learning Objectives
- Describe how psychological disorders are defined, as well as the inherent difficulties in doing so
- Describe the basic features of the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and how it is used to classify disorders
- Discuss historical and supernatural perspectives as well as modern and biological perspectives on the origin of psychological disorders
- Describe the diathesis-stress model and its importance to the study of psychopathology
A psychological disorder is a condition characterized by abnormal thoughts, feelings, and behaviors. Psychopathology is the study of psychological disorders, including their symptoms, etiology (i.e., their causes), and treatment. The term psychopathology can also refer to the manifestation of a psychological disorder. Although consensus can be difficult, it is extremely important for mental health professionals to agree on what kinds of thoughts, feelings, and behaviors are truly abnormal in the sense that they genuinely indicate the presence of psychopathology. Certain patterns of behavior and inner experience can easily be labeled as abnormal and clearly signify some kind of psychological disturbance. The person who washes his hands 40 times per day and the person who claims to hear the voices of demons exhibit behaviors and inner experiences that most would regard as abnormal: beliefs and behaviors that suggest the existence of a psychological disorder. But, consider the nervousness a young man feels when talking to attractive women or the loneliness and longing for home a freshman experiences during her first semester of college—these feelings may not be regularly present, but they fall in the range of normal. So, what kinds of thoughts, feelings, and behaviors represent a true psychological disorder? Psychologists work to distinguish psychological disorders from inner experiences and behaviors that are merely situational, idiosyncratic, or unconventional.
Definition of a Psychological Disorder
Perhaps the simplest approach to conceptualizing psychological disorders is to label behaviors, thoughts, and inner experiences that are atypical, distressful, dysfunctional, and sometimes even dangerous, as signs of a disorder. For example, if you ask a classmate for a date and you are rejected, you probably would feel a little dejected. Such feelings would be normal. If you felt extremely depressed—so much so that you lost interest in activities, had difficulty eating or sleeping, felt utterly worthless, and contemplated suicide—your feelings would be atypical, would deviate from the norm, and could signify the presence of a psychological disorder. Just because something is atypical, however, does not necessarily mean it is disordered.
For example, only about 4% of people in the United States have red hair, so red hair is considered an atypical characteristic (Figure 2), but it is not considered disordered, it’s just unusual. And it is less unusual in Scotland, where approximately 13% of the population has red hair (“DNA Project Aims,” 2012). As you will learn, some disorders, although not exactly typical, are far from atypical, and the rates in which they appear in the population are surprisingly high.

If we can agree that merely being atypical is an insufficient criterion for a having a psychological disorder, is it reasonable to consider behavior or inner experiences that differ from widely expected cultural values or expectations as disordered? Using this criterion, a woman who walks around a subway platform wearing a heavy winter coat in July while screaming obscenities at strangers may be considered as exhibiting symptoms of a psychological disorder. Her actions and clothes violate socially accepted rules governing appropriate dress and behavior; these characteristics are atypical.
Cultural Expectations
Violating cultural expectations is not, in and of itself, a satisfactory means of identifying the presence of a psychological disorder. Since behavior varies from one culture to another, what may be expected and considered appropriate in one culture may not be viewed as such in other cultures. For example, returning a stranger’s smile is expected in the United States because a pervasive social norm dictates that we reciprocate friendly gestures. A person who refuses to acknowledge such gestures might be considered socially awkward—perhaps even disordered—for violating this expectation. However, such expectations are not universally shared. Cultural expectations in Japan involve showing reserve, restraint, and a concern for maintaining privacy around strangers. Japanese people are generally unresponsive to smiles from strangers (Patterson et al., 2007). Eye contact provides another example. In the United States and Europe, eye contact with others typically signifies honesty and attention. However, most Latin-American, Asian, and African cultures interpret direct eye contact as rude, confrontational, and aggressive (Pazain, 2010). Thus, someone who makes eye contact with you could be considered appropriate and respectful or brazen and offensive, depending on your culture (Figure 3).

Hallucinations (seeing or hearing things that are not physically present) in Western societies is a violation of cultural expectations, and a person who reports such inner experiences is readily labeled as psychologically disordered. In other cultures, visions that, for example, pertain to future events may be regarded as normal experiences that are positively valued (Bourguignon, 1970). Finally, it is important to recognize that cultural norms change over time: what might be considered typical in a society at one time may no longer be viewed this way later, similar to how fashion trends from one era may elicit quizzical looks decades later—imagine how a headband, legwarmers, and the big hair of the 1980s would go over on your campus today.
American Psychiatric Association (APA) Definition
Many of the features of the harmful dysfunction model are incorporated in a formal definition of psychological disorder developed by the . According to the American Psychiatric Association (APA) (2013), a psychological disorder is a condition that is said to consist of the following:
- There are significant disturbances in thoughts, feelings, and behaviors. A person must experience inner states (e.g., thoughts and/or feelings) and exhibit behaviors that are clearly disturbed—that is, unusual, but in a negative, self-defeating way. Often, such disturbances are troubling to those around the individual who experiences them. For example, an individual who is uncontrollably preoccupied by thoughts of germs spends hours each day bathing, has inner experiences, and displays behaviors that most would consider atypical and negative (disturbed) and that would likely be troubling to family members.
- The disturbances reflect some kind of biological, psychological, or developmental dysfunction. Disturbed patterns of inner experiences and behaviors should reflect some flaw (dysfunction) in the internal biological, psychological, and developmental mechanisms that lead to normal, healthy psychological functioning. For example, the hallucinations observed in schizophrenia could be a sign of brain abnormalities.
- The disturbances lead to significant distress or disability in one’s life. A person’s inner experiences and behaviors are considered to reflect a psychological disorder if they cause the person considerable distress, or greatly impair his ability to function as a normal individual (often referred to as functional impairment, or occupational and social impairment). As an illustration, a person’s fear of social situations might be so distressing that it causes the person to avoid all social situations (e.g., preventing that person from being able to attend class or apply for a job).
- The disturbances do not reflect expected or culturally approved responses to certain events. Disturbances in thoughts, feelings, and behaviors must be socially unacceptable responses to certain events that often happen in life. For example, it is perfectly natural (and expected) that a person would experience great sadness and might wish to be left alone following the death of a close family member. Because such reactions are in some ways culturally expected, the individual would not be assumed to signify a mental disorder.
Try It
Some believe that there is no essential criterion or set of criteria that can definitively distinguish all cases of disorder from nondisorder (Lilienfeld & Marino, 1999). In truth, no single approach to defining a psychological disorder is adequate by itself, nor is there universal agreement on where the boundary is between disordered and not disordered. From time to time we all experience anxiety, unwanted thoughts, and moments of sadness; our behavior at other times may not make much sense to ourselves or to others. These inner experiences and behaviors can vary in their intensity, but are only considered disordered when they are highly disturbing to us and/or others, suggest a dysfunction in normal mental functioning, and are associated with significant distress or disability in social or occupational activities.
Try It
Think It Over
- Identify a behavior that is considered unusual or abnormal in your own culture that would be considered normal and expected in another culture.
Try It
Diagnosing and Classifying Psychological Disorders
A first step in the study of psychological disorders is carefully and systematically discerning significant signs and symptoms. How do mental health professionals ascertain whether or not a person’s inner states and behaviors truly represent a psychological disorder? Arriving at a proper diagnosis—that is, appropriately identifying and labeling a set of defined symptoms—is absolutely crucial. This process enables professionals to use a common language with others in the field and aids in communication about the disorder with the patient, colleagues and the public. A proper diagnosis is an essential element to guide proper and successful treatment. For these reasons, classification systems that organize psychological disorders systematically are necessary.
Diagnostic And Statistical Manual of Mental Disorders (DSM-5)
Although a number of classification systems have been developed over time, the one that is used by most mental health professionals in the United States is the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), published by the American Psychiatric Association (2013). (Note that the American Psychiatric Association differs from the American Psychological Association; both are abbreviated APA.) The first edition of the DSM, published in 1952, classified psychological disorders according to a format developed by the U.S. Army during World War II (Clegg, 2012). In the years since, the DSM has undergone numerous revisions and editions. The most recent edition, published in 2013, is the DSM-5 (APA, 2013). The DSM-5 includes many categories of disorders (e.g., anxiety disorders, depressive disorders, and dissociative disorders). Each disorder is described in detail, including an overview of the disorder (diagnostic features), specific symptoms required for diagnosis (diagnostic criteria), prevalence information (what percent of the population is thought to be afflicted with the disorder), and risk factors associated with the disorder. Figure 4 shows lifetime prevalence rates—the percentage of people in a population who develop a disorder in their lifetime—of various psychological disorders among U.S. adults. These data were based on a national sample of 9,282 U.S. residents (National Comorbidity Survey, 2007).

The DSM-5 also provides information about comorbidity; the co-occurrence of two disorders. For example, the DSM-5 mentions that 41% of people with obsessive-compulsive disorder (OCD) also meet the diagnostic criteria for major depressive disorder (Figure 5). Drug use is highly comorbid with other mental illnesses; 6 out of 10 people who have a substance use disorder also suffer from another form of mental illness (National Institute on Drug Abuse [NIDA], 2007).

The DSM has changed considerably in the half-century since it was originally published. The first two editions of the DSM, for example, listed homosexuality as a disorder; however, in 1973, the APA voted to remove it from the manual (Silverstein, 2009). Additionally, beginning with the DSM-III in 1980, mental disorders have been described in much greater detail, and the number of diagnosable conditions has grown steadily, as has the size of the manual itself. DSM-I included 106 diagnoses and was 130 total pages, whereas DSM-III included more than 2 times as many diagnoses (265) and was nearly seven times its size (886 total pages) (Mayes & Horowitz, 2005). Although DSM-5 is longer than DSM-IV, the volume includes only 237 disorders, a decrease from the 297 disorders that were listed in DSM-IV. The latest edition, DSM-5, includes revisions in the organization and naming of categories and in the diagnostic criteria for various disorders (Regier, Kuhl, & Kupfer, 2012), while emphasizing careful consideration of the importance of gender and cultural difference in the expression of various symptoms (Fisher, 2010).
Some believe that establishing new diagnoses might overpathologize the human condition by turning common human problems into mental illnesses (The Associated Press, 2013). Indeed, the finding that nearly half of all Americans will meet the criteria for a DSM disorder at some point in their life (Kessler et al., 2005) likely fuels much of this skepticism. The DSM-5 is also criticized on the grounds that its diagnostic criteria have been loosened, thereby threatening to “turn our current diagnostic inflation into diagnostic hyperinflation” (Frances, 2012, para. 22). For example, DSM-IV specified that the symptoms of major depressive disorder must not be attributable to normal bereavement (loss of a loved one). The DSM-5, however, has removed this bereavement exclusion, essentially meaning that grief and sadness after a loved one’s death can constitute major depressive disorder.
Try It
Try It
Compassionate View of Psychological Disorders
As these disorders are outlined, please bear two things in mind. First, remember that psychological disorders represent extremes of inner experience and behavior. If, while reading about these disorders, you feel that these descriptions begin to personally characterize you, do not worry—this moment of enlightenment probably means nothing more than you are normal. Each of us experiences episodes of sadness, anxiety, and preoccupation with certain thoughts—times when we do not quite feel ourselves. These episodes should not be considered problematic unless the accompanying thoughts and behaviors become extreme and have a disruptive effect on one’s life. Second, understand that people with psychological disorders are far more than just embodiments of their disorders. We do not use terms such as schizophrenics, depressives, or phobics because they are labels that objectify people who suffer from these conditions, thus promoting biased and disparaging assumptions about them. It is important to remember that a psychological disorder is not what a person is; it is something that a person has—through no fault of his or her own. As is the case with cancer or diabetes, those with psychological disorders suffer debilitating, often painful conditions that are not of their own choosing. These individuals deserve to be viewed and treated with compassion, understanding, and dignity.
Watch It
Watch this CrashCourse Psychology video to better understand the history of diagnosing psychological disorders and how they are classified.
Try It
Perspectives on Psychological Disorders
Supernatural Perspectives of Psychological Disorders
For centuries, psychological disorders were viewed from a supernatural perspective: attributed to a force beyond scientific understanding. Those afflicted were thought to be practitioners of black magic or possessed by spirits (Maher & Maher, 1985). For example, convents throughout Europe in the 16th and 17th centuries reported hundreds of nuns falling into a state of frenzy in which the afflicted foamed at the mouth, screamed and convulsed, sexually propositioned priests, and confessed to having carnal relations with devils or Christ. Although, today, these cases would suggest serious mental illness; at the time, these events were routinely explained as possession by devilish forces (Waller, 2009a). Similarly, grievous fits by young girls are believed to have precipitated the witch panic in New England late in the 17th century (Demos, 1983). Such beliefs in supernatural causes of mental illness are still held in some societies today; for example, beliefs that supernatural forces cause mental illness are common in some cultures in modern-day Nigeria (Aghukwa, 2012).
Biological Perspectives of Psychological Disorders

Findings such as these have led many of today’s researchers to search for specific genes and genetic mutations that contribute to mental disorders. Also, sophisticated neural imaging technology in recent decades has revealed how abnormalities in brain structure and function might be directly involved in many disorders, and advances in our understanding of neurotransmitters and hormones have yielded insights into their possible connections. The biological perspective is currently thriving in the study of psychological disorders.
Diathesis-Stress Model of Psychological Disorders
Despite advances in understanding the biological basis of psychological disorders, the psychosocial perspective is still very important. This perspective emphasizes the importance of learning, stress, faulty and self-defeating thinking patterns, and environmental factors. Perhaps the best way to think about psychological disorders, then, is to view them as originating from a combination of biological and psychological processes. Many develop not from a single cause, but from a delicate fusion between partly biological and partly psychosocial factors.
The diathesis-stress model (Zuckerman, 1999) integrates biological and psychosocial factors to predict the likelihood of a disorder. This diathesis-stress model suggests that people with an underlying predisposition for a disorder (i.e., a diathesis) are more likely than others to develop a disorder when faced with adverse environmental or psychological events (i.e., stress), such as childhood maltreatment, negative life events, trauma, and so on. A diathesis is not always a biological vulnerability to an illness; some diatheses may be psychological (e.g., a tendency to think about life events in a pessimistic, self-defeating way).
The key assumption of the diathesis-stress model is that both factors, diathesis and stress, are necessary in the development of a disorder. Different models explore the relationship between the two factors: the level of stress needed to produce the disorder is inversely proportional to the level of diathesis.
Try It
Think It Over
- Even today, some believe that certain occurrences have supernatural causes. Think of an event, recent or historical, for which others have provided supernatural explanation.
Try It
Anxiety Disorders, Obsessive-Compulsive Disorder, and Posttraumatic Stress Disorder
 In this section you will learn about anxiety disorders and other related disorders:
In this section you will learn about anxiety disorders and other related disorders:
- Anxiety disorders are a group of disorders in which a person experiences excessive, persistent, and distressing fear and anxiety that interferes with normal functioning. Anxiety disorders include specific phobia: a specific unrealistic fear; social anxiety disorder: extreme fear and avoidance of social situations; panic disorder: suddenly overwhelmed by panic even though there is no apparent reason to be frightened; agoraphobia: an intense fear and avoidance of situations in which it might be difficult to escape; and generalized anxiety disorder: a relatively continuous state of tension, apprehension, and dread.
- Obsessive-compulsive and related disorders like body dysmorphic disorder or hoarding are a group of DSM-5 disorders that overlap somewhat in that they each involve intrusive thoughts and/or repetitive behaviors that also typically cause anxiousness. Perhaps the most recognized of these disorders is obsessive-compulsive disorder, in which a person is obsessed with unwanted, unpleasant thoughts and/or compulsively engages in repetitive behaviors or mental acts, perhaps as a way of coping with the obsessions.
- Although related to anxiety disorders, posttraumatic stress disorder is now classified as a “Trauma-and-Stressor-Related Disorder.” PTSD is defined as a disorder in which the experience of a traumatic or profoundly stressful event, such as combat, sexual assault, or natural disaster, produces a constellation of symptoms that must last for one month or more. These symptoms include intrusive and distressing memories of the event, flashbacks, avoidance of stimuli or situations that are connected to the event, persistently negative emotional states, feeling detached from others, irritability, proneness toward outbursts, and a tendency to be easily startled. Not everyone who experiences a traumatic event will develop PTSD; a variety of risk factors associated with its development have been identified.
Anxiety Disorders, Obsessive-Compulsive Disorder, and Posttraumatic Stress Disorder
Learning Objectives
- Distinguish normal anxiety from pathological anxiety
- Explain phobias and their acquisition through learning
- Describe the main features of social anxiety disorder
- Explain panic disorder and panic attacks
- Describe the symptoms and prevalence of generalized anxiety disorder
- Describe the main features, development, and prevalence of obsessive-compulsive disorder, body dysmorphic disorder, and hoarding disorder
- Describe the nature, development, symptoms, and risk factors associated with posttraumatic stress disorder
Phobias and Social Anxiety Disorder
Everybody experiences anxiety from time to time. Although anxiety is closely related to fear, the two states possess important differences. Fear involves an instantaneous reaction to an imminent threat, whereas anxiety involves apprehension, avoidance, and cautiousness regarding a potential threat, danger, or other negative event (Craske, 1999). While anxiety is unpleasant to most people, it is important to our health, safety, and well-being. Anxiety motivates us to take actions—such as preparing for exams, watching our weight, showing up to work on time—that enable us to avert potential future problems. Anxiety also motivates us to avoid certain things—such as running up debts and engaging in illegal activities—that could lead to future trouble. Most individuals’ level and duration of anxiety approximates the magnitude of the potential threat they face. For example, suppose a single woman in her late 30s who wishes to marry is concerned about the possibility of having to settle for a spouse who is less attractive and educated than desired. This woman likely would experience anxiety of greater intensity and duration than would a 21-year-old college junior who is having trouble finding a date for the annual social. Some people, however, experience anxiety that is excessive, persistent, and greatly out of proportion to the actual threat; if one’s anxiety has a disruptive influence on one’s live, this is a strong indicator that the individual is experiencing an anxiety disorder.

Anxiety disorders are characterized by excessive and persistent fear and anxiety, and by related disturbances in behavior (APA, 2013). Although anxiety is universally experienced, anxiety disorders cause considerable distress. As a group, anxiety disorders are common: approximately 25%–30% of the U.S. population meets the criteria for at least one anxiety disorder during their lifetime (Kessler et al., 2005). Also, these disorders appear to be much more common in women than they are in men; within a 12-month period, around 23% of women and 14% of men will experience at least one anxiety disorder (National Comorbidity Survey, 2007). Anxiety disorders are the most frequently occurring class of mental disorders and are often comorbid with each other and with other mental disorders (Kessler, Ruscio, Shear, & Wittchen, 2009).
Specific Phobia
Phobia is a Greek word that means fear. A person diagnosed with a specific phobia (formerly known as simple phobia) experiences excessive, distressing, and persistent fear or anxiety about a specific object or situation (such as animals, enclosed spaces, elevators, or flying) (APA, 2013). Even though people realize their level of fear and anxiety in relation to the phobic stimulus is irrational, some people with a specific phobia may go to great lengths to avoid the phobic stimulus (the object or situation that triggers the fear and anxiety). Typically, the fear and anxiety a phobic stimulus elicits is disruptive to the person’s life. For example, a man with a phobia of flying might refuse to accept a job that requires frequent air travel, thus negatively affecting his career. Clinicians who have worked with people who have specific phobias have encountered many kinds of phobias, some of which are shown in Table 1.
| Phobia | Feared Object or Situation |
|---|---|
| Acrophobia | heights |
| Aerophobia | flying |
| Arachnophobia | spiders |
| Claustrophobia | enclosed spaces |
| Cynophobia | dogs |
| Hematophobia | blood |
| Ophidiophobia | snakes |
| Taphophobia | being buried alive |
| Trypanophobia | injections |
| Xenophobia | strangers |

Specific phobias are common; in the United States, around 12.5% of the population will meet the criteria for a specific phobia at some point in their lifetime (Kessler et al., 2005). One type of phobia, agoraphobia, is listed in the DSM-5 as a separate anxiety disorder. Agoraphobia, which literally means “fear of the marketplace,” is characterized by intense fear, anxiety, and avoidance of situations in which it might be difficult to escape or receive help if one experiences symptoms of a panic attack (a state of extreme anxiety that we will discuss shortly). These situations include public transportation, open spaces (parking lots), enclosed spaces (stores), crowds, or being outside the home alone (APA, 2013). About 1.4% of Americans experience agoraphobia during their lifetime (Kessler et al., 2005).
Acquisition of Phobias Through Learning
Many theories suggest that phobias develop through learning. Rachman (1977) proposed that phobias can be acquired through three major learning pathways. The first pathway is through classical conditioning. As you may recall, classical conditioning is a form of learning in which a previously neutral stimulus is paired with an unconditioned stimulus (UCS) that reflexively elicits an unconditioned response (UCR), eliciting the same response through its association with the unconditioned stimulus. The response is called a conditioned response (CR). For example, a child who has been bitten by a dog may come to fear dogs because of her past association with pain. In this case, the dog bite is the UCS and the fear it elicits is the UCR. Because a dog was associated with the bite, any dog may come to serve as a conditioned stimulus, thereby eliciting fear; the fear the child experiences around dogs, then, becomes a CR.
The second pathway of phobia acquisition is through vicarious learning, such as modeling. For example, a child who observes his cousin react fearfully to spiders may later express the same fears, even though spiders have never presented any danger to him. This phenomenon has been observed in both humans and nonhuman primates (Olsson & Phelps, 2007). A study of laboratory-reared monkeys readily acquired a fear of snakes after observing wild-reared monkeys react fearfully to snakes (Mineka & Cook, 1993).
The third pathway is through verbal transmission or information. For example, a child whose parents, siblings, friends, and classmates constantly tell her how disgusting and dangerous snakes are may come to acquire a fear of snakes.
Interestingly, people are more likely to develop phobias of things that do not represent much actual danger to themselves, such as animals and heights, and are less likely to develop phobias toward things that present legitimate danger in contemporary society, such as motorcycles and weapons (Öhman & Mineka, 2001). Why might this be so? One theory suggests that the human brain is evolutionarily predisposed to more readily associate certain objects or situations with fear (Seligman, 1971). This theory argues that throughout our evolutionary history, our ancestors associated certain stimuli (e.g., snakes, spiders, heights, and thunder) with potential danger. As time progressed, the mind has become adapted to more readily develop fears of these things than of others. Experimental evidence has consistently demonstrated that conditioned fears develop more readily to fear-relevant stimuli (images of snakes and spiders) than to fear-irrelevant stimuli (images of flowers and berries) (Öhman & Mineka, 2001). Such prepared learning has also been shown to occur in monkeys. In one study (Cook & Mineka, 1989), monkeys watched videotapes of model monkeys reacting fearfully to either fear-relevant stimuli (toy snakes or a toy crocodile) or fear-irrelevant stimuli (flowers or a toy rabbit). The observer monkeys developed fears of the fear-relevant stimuli but not the fear-irrelevant stimuli.
Try It
Social Anxiety Disorder
Social anxiety disorder (formerly called social phobia) is characterized by extreme and persistent fear or anxiety and avoidance of social situations in which the person could potentially be evaluated negatively by others (APA, 2013). As with specific phobias, social anxiety disorder is common in the United States; a little over 12% of all Americans experience social anxiety disorder during their lifetime (Kessler et al., 2005).
The heart of the fear and anxiety in social anxiety disorder is the person’s concern that he may act in a humiliating or embarrassing way, such as appearing foolish, showing symptoms of anxiety (blushing), or doing or saying something that might lead to rejection (such as offending others). The kinds of social situations in which individuals with social anxiety disorder usually have problems include public speaking, having a conversation, meeting strangers, eating in restaurants, and, in some cases, using public restrooms. Although many people become anxious in social situations like public speaking, the fear, anxiety, and avoidance experienced in social anxiety disorder are highly distressing and lead to serious impairments in life. Adults with this disorder are more likely to experience lower educational attainment and lower earnings (Katzelnick et al., 2001), perform more poorly at work and are more likely to be unemployed (Moitra, Beard, Weisberg, & Keller, 2011), and report greater dissatisfaction with their family lives, friends, leisure activities, and income (Stein & Kean, 2000).
When people with social anxiety disorder are unable to avoid situations that provoke anxiety, they typically perform safety behaviors: mental or behavioral acts that reduce anxiety in social situations by reducing the chance of negative social outcomes. Safety behaviors include avoiding eye contact, rehearsing sentences before speaking, talking only briefly, and not talking about oneself (Alden & Bieling, 1998). Other examples of safety behaviors include the following (Marker, 2013):
- assuming roles in social situations that minimize interaction with others (e.g., taking pictures, setting up equipment, or helping prepare food)
- asking people many questions to keep the focus off of oneself
- selecting a position to avoid scrutiny or contact with others (sitting in the back of the room)
- wearing bland, neutral clothes to avoid drawing attention to oneself
- avoiding substances or activities that might cause anxiety symptoms (such as caffeine, warm clothing, and physical exercise)
Although these behaviors are intended to prevent the person with social anxiety disorder from doing something awkward that might draw criticism, these actions usually exacerbate the problem because they do not allow the individual to disconfirm his negative beliefs, often eliciting rejection and other negative reactions from others (Alden & Bieling, 1998).
Try It
People with social anxiety disorder may resort to self-medication, such as drinking alcohol, as a means to avert the anxiety symptoms they experience in social situations (Battista & Kocovski, 2010). The use of alcohol when faced with such situations may become negatively reinforcing: encouraging individuals with social anxiety disorder to turn to the substance whenever they experience anxiety symptoms. The tendency to use alcohol as a coping mechanism for social anxiety, however, can come with a hefty price tag: a number of large scale studies have reported a high rate of comorbidity between social anxiety disorder and alcohol use disorder (Morris, Stewart, & Ham, 2005).
As with specific phobias, it is highly probable that the fears inherent to social anxiety disorder can develop through conditioning experiences. For example, a child who is subjected to early unpleasant social experiences (e.g., bullying at school) may develop negative social images of herself that become activated later in anxiety-provoking situations (Hackmann, Clark, & McManus, 2000). Indeed, one study reported that 92% of a sample of adults with social anxiety disorder reported a history of severe teasing in childhood, compared to only 35% of a sample of adults with panic disorder (McCabe, Antony, Summerfeldt, Liss, & Swinson, 2003).
One of the most well-established risk factors for developing social anxiety disorder is behavioral inhibition (Clauss & Blackford, 2012). Behavioral inhibition is thought to be an inherited trait, and it is characterized by a consistent tendency to show fear and restraint when presented with unfamiliar people or situations (Kagan, Reznick, & Snidman, 1988). Behavioral inhibition is displayed very early in life; behaviorally inhibited toddlers and children respond with great caution and restraint in unfamiliar situations, and they are often timid, fearful, and shy around unfamiliar people (Fox, Henderson, Marshall, Nichols, & Ghera, 2005). A recent statistical review of studies demonstrated that behavioral inhibition was associated with more than a sevenfold increase in the risk of development of social anxiety disorder, demonstrating that behavioral inhibition is a major risk factor for the disorder (Clauss & Blackford, 2012).
Try It
Panic Disorder
Imagine that you are at the mall one day with your friends and—suddenly and inexplicably—you begin sweating and trembling, your heart starts pounding, you have trouble breathing, and you start to feel dizzy and nauseous. This episode lasts for 10 minutes and is terrifying because you start to think that you are going to die. When you visit your doctor the following morning and describe what happened, she tells you that you have experienced a panic attack (Figure 9). If you experience another one of these episodes two weeks later and worry for a month or more that similar episodes will occur in the future, it is likely that you have developed panic disorder.

People with panic disorder experience recurrent (more than one) and unexpected panic attacks, along with at least one month of persistent concern about additional panic attacks, worry over the consequences of the attacks, or self-defeating changes in behavior related to the attacks (e.g., avoidance of exercise or unfamiliar situations) (APA, 2013). As is the case with other anxiety disorders, the panic attacks cannot result from the physiological effects of drugs and other substances, a medical condition, or another mental disorder. A panic attack is defined as a period of extreme fear or discomfort that develops abruptly and reaches a peak within 10 minutes. Its symptoms include accelerated heart rate, sweating, trembling, choking sensations, hot flashes or chills, dizziness or lightheadedness, fears of losing control or going crazy, and fears of dying (APA, 2013). Sometimes panic attacks are expected, occurring in response to specific environmental triggers (such as being in a tunnel); other times, these episodes are unexpected and emerge randomly (such as when relaxing). According to the DSM-5, the person must experience unexpected panic attacks to qualify for a diagnosis of panic disorder.
Experiencing a panic attack is often terrifying. Rather than recognizing the symptoms of a panic attack merely as signs of intense anxiety, individuals with panic disorder often misinterpret them as a sign that something is intensely wrong internally (thinking, for example, that the pounding heart represents an impending heart attack). Panic attacks can occasionally precipitate trips to the emergency room because several symptoms of panic attacks are, in fact, similar to those associated with heart problems (e.g., palpitations, racing pulse, and a pounding sensation in the chest) (Root, 2000). Unsurprisingly, those with panic disorder fear future attacks and may become preoccupied with modifying their behavior in an effort to avoid future panic attacks. For this reason, panic disorder is often characterized as fear of fear (Goldstein & Chambless, 1978).
Panic attacks themselves are not mental disorders. Indeed, around 23% of Americans experience isolated panic attacks in their lives without meeting the criteria for panic disorder (Kessler et al., 2006), indicating that panic attacks are fairly common. Panic disorder is, of course, much less common, afflicting 4.7% of Americans during their lifetime (Kessler et al., 2005). Many people with panic disorder develop agoraphobia, which is marked by fear and avoidance of situations in which escape might be difficult or help might not be available if one were to develop symptoms of a panic attack. People with panic disorder often experience a comorbid disorder, such as other anxiety disorders or major depressive disorder (APA, 2013).
Try It
Researchers are not entirely sure what causes panic disorder. Children are at a higher risk of developing panic disorder if their parents have the disorder (Biederman et al., 2001), and family and twins studies indicate that the heritability of panic disorder is around 43% (Hettema, Neale, & Kendler, 2001). The exact genes and gene functions involved in this disorder, however, are not well-understood (APA, 2013). Neurobiological theories of panic disorder suggest that a region of the brain called the locus coeruleus may play a role in this disorder. Located in the brainstem, the locus coeruleus is the brain’s major source of norepinephrine, a neurotransmitter that triggers the body’s fight-or-flight response. Activation of the locus coeruleus is associated with anxiety and fear, and research with nonhuman primates has shown that stimulating the locus coeruleus either electrically or through drugs produces panic-like symptoms (Charney et al., 1990). Such findings have led to the theory that panic disorder may be caused by abnormal norepinephrine activity in the locus coeruleus (Bremner, Krystal, Southwick, & Charney, 1996).
Conditioning theories of panic disorder propose that panic attacks are classical conditioning responses to subtle bodily sensations resembling those normally occurring when one is anxious or frightened (Bouton, Mineka, & Barlow, 2001). For example, consider a child who has asthma. An acute asthma attack produces sensations, such as shortness of breath, coughing, and chest tightness, that typically elicit fear and anxiety. Later, when the child experiences subtle symptoms that resemble the frightening symptoms of earlier asthma attacks (such as shortness of breath after climbing stairs), he may become anxious, fearful, and then experience a panic attack. In this situation, the subtle symptoms would represent a conditioned stimulus, and the panic attack would be a conditioned response. The finding that panic disorder is nearly three times as frequent among people with asthma as it is among people without asthma (Weiser, 2007) supports the possibility that panic disorder has the potential to develop through classical conditioning.
Cognitive factors may play an integral part in panic disorder. Generally, cognitive theories (Clark, 1996) argue that those with panic disorder are prone to interpret ordinary bodily sensations catastrophically, and these fearful interpretations set the stage for panic attacks. For example, a person might detect bodily changes that are routinely triggered by innocuous events such getting up from a seated position (dizziness), exercising (increased heart rate, shortness of breath), or drinking a large cup of coffee (increased heart rate, trembling). The individual interprets these subtle bodily changes catastrophically (“Maybe I’m having a heart attack!”). Such interpretations create fear and anxiety, which trigger additional physical symptoms; subsequently, the person experiences a panic attack. Support of this contention rests with findings that people with more severe catastrophic thoughts about sensations have more frequent and severe panic attacks, and among those with panic disorder, reducing catastrophic cognitions about their sensations is as effective as medication in reducing panic attacks (Good & Hinton, 2009).
Try It
Generalized Anxiety Disorder
Alex was always worried about many things. He worried that his children would drown when they played at the beach. Each time he left the house, he worried that an electrical short circuit would start a fire in his home. He worried that his wife would lose her job at the prestigious law firm. He worried that his daughter’s minor staph infection could turn into a massive life-threatening condition. These and other worries constantly weighed heavily on Alex’s mind, so much so that they made it difficult for him to make decisions and often left him feeling tense, irritable, and worn out. One night, Alex’s wife was to drive their son home from a soccer game. However, his wife stayed after the game and talked with some of the other parents, resulting in her arriving home 45 minutes late. Alex had tried to call his cell phone three or four times, but he could not get through because the soccer field did not have a signal. Extremely worried, Alex eventually called the police, convinced that his wife and son had not arrived home because they had been in a terrible car accident.
Alex suffers from generalized anxiety disorder: a relatively continuous state of excessive, uncontrollable, and pointless worry and apprehension. People with generalized anxiety disorder often worry about routine, everyday things, even though their concerns are unjustified (Figure 10). For example, an individual may worry about her health and finances, the health of family members, the safety of her children, or minor matters (e.g., being late for an appointment) without having any legitimate reason for doing so (APA, 2013). A diagnosis of generalized anxiety disorder requires that the diffuse worrying and apprehension characteristic of this disorder—what Sigmund Freud referred to as free-floating anxiety—is not part of another disorder, occurs more days than not for at least six months, and is accompanied by any three of the following symptoms: restlessness, difficulty concentrating, being easily fatigued, muscle tension, irritability, and sleep difficulties.

About 5.7% of the U.S. population will develop symptoms of generalized anxiety disorder during their lifetime (Kessler et al., 2005), and females are 2 times as likely as males to experience the disorder (APA, 2013). Generalized anxiety disorder is highly comorbid with mood disorders and other anxiety disorders (Noyes, 2001), and it tends to be chronic. Also, generalized anxiety disorder appears to increase the risk for heart attacks and strokes, especially in people with preexisting heart conditions (Martens et al., 2010).
Although there have been few investigations aimed at determining the heritability of generalized anxiety disorder, a summary of available family and twin studies suggests that genetic factors play a modest role in the disorder (Hettema et al., 2001). Cognitive theories of generalized anxiety disorder suggest that worry represents a mental strategy to avoid more powerful negative emotions (Aikins & Craske, 2001), perhaps stemming from earlier unpleasant or traumatic experiences. Indeed, one longitudinal study found that childhood maltreatment was strongly related to the development of this disorder during adulthood (Moffitt et al., 2007); worrying might distract people from remembering painful childhood experiences.
Try It
Obsessive-Compulsive and Related Disorders
Obsessive-compulsive and related disorders are a group of overlapping disorders that generally involve intrusive, unpleasant thoughts and repetitive behaviors. Many of us experience unwanted thoughts from time to time (e.g., craving double cheeseburgers when dieting), and many of us engage in repetitive behaviors on occasion (e.g., pacing when nervous). However, obsessive-compulsive and related disorders elevate the unwanted thoughts and repetitive behaviors to a status so intense that these cognitions and activities disrupt daily life. Included in this category are obsessive-compulsive disorder (OCD), body dysmorphic disorder, and hoarding disorder.
Obsessive-Compulsive Disorders
People with obsessive-compulsive disorder (OCD) experience thoughts and urges that are intrusive and unwanted (obsessions) and/or the need to engage in repetitive behaviors or mental acts (compulsions). A person with this disorder might, for example, spend hours each day washing his hands or constantly checking and rechecking to make sure that a stove, faucet, or light has been turned off.
Obsessions are more than just unwanted thoughts that seem to randomly jump into our head from time to time, such as recalling an insensitive remark a coworker made recently, and they are more significant than day-to-day worries we might have, such as justifiable concerns about being laid off from a job. Rather, obsessions are characterized as persistent, unintentional, and unwanted thoughts and urges that are highly intrusive, unpleasant, and distressing (APA, 2013). Common obsessions include concerns about germs and contamination, doubts (“Did I turn the water off?”), order and symmetry (“I need all the spoons in the tray to be arranged a certain way”), and urges that are aggressive or lustful. Usually, the person knows that such thoughts and urges are irrational and thus tries to suppress or ignore them, but has an extremely difficult time doing so. These obsessive symptoms sometimes overlap, such that someone might have both contamination and aggressive obsessions (Abramowitz & Siqueland, 2013).
Compulsions are repetitive and ritualistic acts that are typically carried out primarily as a means to minimize the distress that obsessions trigger or to reduce the likelihood of a feared event (APA, 2013). Compulsions often include such behaviors as repeated and extensive hand washing, cleaning, checking (e.g., that a door is locked), and ordering (e.g., lining up all the pencils in a particular way), and they also include such mental acts as counting, praying, or reciting something to oneself (Figure 11). Compulsions characteristic of OCD are not performed out of pleasure, nor are they connected in a realistic way to the source of the distress or feared event. Approximately 2.3% of the U.S. population will experience OCD in their lifetime (Ruscio, Stein, Chiu, & Kessler, 2010) and, if left untreated, OCD tends to be a chronic condition creating lifelong interpersonal and psychological problems (Norberg, Calamari, Cohen, & Riemann, 2008).
Try It
Watch It
Watch this video to understand why people who are simply orderly or meticulous are probably not suffering from obsessive-compulsive disorder.
You can view the transcript for “Debunking the myths of OCD – Natasha M. Santos” here (opens in new window).

Body Dysmorphic Disorder
An individual with body dysmorphic disorder is preoccupied with a perceived flaw in her physical appearance that is either nonexistent or barely noticeable to other people (APA, 2013). These perceived physical defects cause the person to think she is unattractive, ugly, hideous, or deformed. These preoccupations can focus on any bodily area, but they typically involve the skin, face, or hair. The preoccupation with imagined physical flaws drives the person to engage in repetitive and ritualistic behavioral and mental acts, such as constantly looking in the mirror, trying to hide the offending body part, comparisons with others, and, in some extreme cases, cosmetic surgery (Phillips, 2005). An estimated 2.4% of the adults in the United States meet the criteria for body dysmorphic disorder, with slightly higher rates in women than in men (APA, 2013).
Hoarding Disorder
Although hoarding was traditionally considered to be a symptom of OCD, considerable evidence suggests that hoarding represents an entirely different disorder (Mataix-Cols et al., 2010). People with hoarding disorder cannot bear to part with personal possessions, regardless of how valueless or useless these possessions are. As a result, these individuals accumulate excessive amounts of usually worthless items that clutter their living areas (Figure 12). Often, the quantity of cluttered items is so excessive that the person is unable use his kitchen, or sleep in his bed. People who suffer from this disorder have great difficulty parting with items because they believe the items might be of some later use, or because they form a sentimental attachment to the items (APA, 2013). Importantly, a diagnosis of hoarding disorder is made only if the hoarding is not caused by another medical condition and if the hoarding is not a symptom of another disorder (e.g., schizophrenia) (APA, 2013).

Causes of OCD
The results of family and twin studies suggest that OCD has a moderate genetic component. The disorder is five times more frequent in the first-degree relatives of people with OCD than in people without the disorder (Nestadt et al., 2000). Additionally, the concordance rate of OCD among identical twins is around 57%; however, the concordance rate for fraternal twins is 22% (Bolton, Rijsdijk, O’Connor, Perrin, & Eley, 2007). Studies have implicated about two dozen potential genes that may be involved in OCD; these genes regulate the function of three neurotransmitters: serotonin, dopamine, and glutamate (Pauls, 2010). Many of these studies included small sample sizes and have yet to be replicated. Thus, additional research needs to be done in this area.
A brain region that is believed to play a critical role in OCD is the orbitofrontal cortex (Kopell & Greenberg, 2008), an area of the frontal lobe involved in learning and decision-making (Rushworth, Noonan, Boorman, Walton, & Behrens, 2011) (Figure 13). In people with OCD, the orbitofrontal cortex becomes especially hyperactive when they are provoked with tasks in which, for example, they are asked to look at a photo of a toilet or of pictures hanging crookedly on a wall (Simon, Kaufmann, Müsch, Kischkel, & Kathmann, 2010). The orbitofrontal cortex is part of a series of brain regions that, collectively, is called the OCD circuit; this circuit consists of several interconnected regions that influence the perceived emotional value of stimuli and the selection of both behavioral and cognitive responses (Graybiel & Rauch, 2000). As with the orbitofrontal cortex, other regions of the OCD circuit show heightened activity during symptom provocation (Rotge et al., 2008), which suggests that abnormalities in these regions may produce the symptoms of OCD (Saxena, Bota, & Brody, 2001). Consistent with this explanation, people with OCD show a substantially higher degree of connectivity of the orbitofrontal cortex and other regions of the OCD circuit than do those without OCD (Beucke et al., 2013).

The findings discussed above were based on imaging studies, and they highlight the potential importance of brain dysfunction in OCD. However, one important limitation of these findings is the inability to explain differences in obsessions and compulsions. Another limitation is that the correlational relationship between neurological abnormalities and OCD symptoms cannot imply causation (Abramowitz & Siqueland, 2013).
Watch It
Watch this CrashCourse psychology video to learn about the accurate definitions of phobias and OCD and how these contrast with common, incorrect descriptions of the terms.
Connect the Concepts: Conditioning and OCD
The symptoms of OCD have been theorized to be learned responses, acquired and sustained as the result of a combination of two forms of learning: classical conditioning and operant conditioning (Mowrer, 1960; Steinmetz, Tracy, & Green, 2001). Specifically, the acquisition of OCD may occur first as the result of classical conditioning, whereby a neutral stimulus becomes associated with an unconditioned stimulus that provokes anxiety or distress. When an individual has acquired this association, subsequent encounters with the neutral stimulus trigger anxiety, including obsessive thoughts; the anxiety and obsessive thoughts (which are now a conditioned response) may persist until she identifies some strategy to relieve it. Relief may take the form of a ritualistic behavior or mental activity that, when enacted repeatedly, reduces the anxiety. Such efforts to relieve anxiety constitute an example of negative reinforcement (a form of operant conditioning). Recall from the chapter on learning that negative reinforcement involves the strengthening of behavior through its ability to remove something unpleasant or aversive. Hence, compulsive acts observed in OCD may be sustained because they are negatively reinforcing, in the sense that they reduce anxiety triggered by a conditioned stimulus.
Suppose an individual with OCD experiences obsessive thoughts about germs, contamination, and disease whenever she encounters a doorknob. What might have constituted a viable unconditioned stimulus? Also, what would constitute the conditioned stimulus, unconditioned response, and conditioned response? What kinds of compulsive behaviors might we expect, and how do they reinforce themselves? What is decreased? Additionally, and from the standpoint of learning theory, how might the symptoms of OCD be treated successfully?
Try It
Posttraumatic Stress Disorder
Extremely stressful or traumatic events, such as combat, natural disasters, and terrorist attacks, place the people who experience them at an increased risk for developing psychological disorders such as posttraumatic stress disorder (PTSD). Throughout much of the 20th century, this disorder was called shell shock and combat neurosis because its symptoms were observed in soldiers who had engaged in wartime combat. By the late 1970s it had become clear that women who had experienced sexual traumas (e.g., rape, domestic battery, and incest) often experienced the same set of symptoms as did soldiers (Herman, 1997). The term posttraumatic stress disorder was developed given that these symptoms could happen to anyone who experienced psychological trauma.
A Broader Definition of PTSD
PTSD was listed among the anxiety disorders in previous DSM editions. In DSM-5, it is now listed among a group called Trauma-and-Stressor-Related Disorders. For a person to be diagnosed with PTSD, she be must exposed to, witness, or experience the details of a traumatic experience (e.g., a first responder), one that involves “actual or threatened death, serious injury, or sexual violence” (APA, 2013, p. 271). These experiences can include such events as combat, threatened or actual physical attack, sexual assault, natural disasters, terrorist attacks, and automobile accidents. This criterion makes PTSD the only disorder listed in the DSM in which a cause (extreme trauma) is explicitly specified.
Symptoms of PTSD include intrusive and distressing memories of the event, flashbacks (states that can last from a few seconds to several days, during which the individual relives the event and behaves as if the event were occurring at that moment [APA, 2013]), avoidance of stimuli connected to the event, persistently negative emotional states (e.g., fear, anger, guilt, and shame), feelings of detachment from others, irritability, proneness toward outbursts, and an exaggerated startle response (jumpiness). For PTSD to be diagnosed, these symptoms must occur for at least one month.
Roughly 7% of adults in the United States, including 9.7% of women and 3.6% of men, experience PTSD in their lifetime (National Comorbidity Survey, 2007), with higher rates among people exposed to mass trauma and people whose jobs involve duty-related trauma exposure (e.g., police officers, firefighters, and emergency medical personnel) (APA, 2013). Nearly 21% of residents of areas affected by Hurricane Katrina suffered from PTSD one year following the hurricane (Kessler et al., 2008), and 12.6% of Manhattan residents were observed as having PTSD 2–3 years after the 9/11 terrorist attacks (DiGrande et al., 2008).
Try It
Risk Factors for PTSD
Of course, not everyone who experiences a traumatic event will go on to develop PTSD; several factors strongly predict the development of PTSD: trauma experience, greater trauma severity, lack of immediate social support, and more subsequent life stress (Brewin, Andrews, & Valentine, 2000). Traumatic events that involve harm by others (e.g., combat, rape, and sexual molestation) carry greater risk than do other traumas (e.g., natural disasters) (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). Factors that increase the risk of PTSD include female gender, low socioeconomic status, low intelligence, personal history of mental disorders, history of childhood adversity (abuse or other trauma during childhood), and family history of mental disorders (Brewin et al., 2000). Personality characteristics such as neuroticism and somatization (the tendency to experience physical symptoms when one encounters stress) have been shown to elevate the risk of PTSD (Bramsen, Dirkzwager, & van der Ploeg, 2000). People who experience childhood adversity and/or traumatic experiences during adulthood are at significantly higher risk of developing PTSD if they possess one or two short versions of a gene that regulates the neurotransmitter serotonin (Xie et al., 2009). This suggests a possible diathesis-stress interpretation of PTSD: its development is influenced by the interaction of psychosocial and biological factors.
Support for Sufferers of PTSD
Research has shown that social support following a traumatic event can reduce the likelihood of PTSD (Ozer, Best, Lipsey, & Weiss, 2003). Social support is often defined as the comfort, advice, and assistance received from relatives, friends, and neighbors. Social support can help individuals cope during difficult times by allowing them to discuss feelings and experiences and providing a sense of being loved and appreciated. A 14-year study of 1,377 American Legionnaires who had served in the Vietnam War found that those who perceived less social support when they came home were more likely to develop PTSD than were those who perceived greater support (Figure 14). In addition, those who became involved in the community were less likely to develop PTSD, and they were more likely to experience a remission of PTSD than were those who were less involved (Koenen, Stellman, Stellman, & Sommer, 2003).

Learning and Development of PTSD
PTSD learning models suggest that some symptoms are developed and maintained through classical conditioning. The traumatic event may act as an unconditioned stimulus that elicits an unconditioned response characterized by extreme fear and anxiety. Cognitive, emotional, physiological, and environmental cues accompanying or related to the event are conditioned stimuli. These traumatic reminders evoke conditioned responses (extreme fear and anxiety) similar to those caused by the event itself (Nader, 2001). A person who was in the vicinity of the Twin Towers during the 9/11 terrorist attacks and who developed PTSD may display excessive hypervigilance and distress when planes fly overhead; this behavior constitutes a conditioned response to the traumatic reminder (conditioned stimulus of the sight and sound of an airplane). Differences in how conditionable individuals are help to explain differences in the development and maintenance of PTSD symptoms (Pittman, 1988). Conditioning studies demonstrate facilitated acquisition of conditioned responses and delayed extinction of conditioned responses in people with PTSD (Orr et al., 2000).
Cognitive factors are important in the development and maintenance of PTSD. One model suggests that two key processes are crucial: disturbances in memory for the event, and negative appraisals of the trauma and its aftermath (Ehlers & Clark, 2000). According to this theory, some people who experience traumas do not form coherent memories of the trauma; memories of the traumatic event are poorly encoded and, thus, are fragmented, disorganized, and lacking in detail. Therefore, these individuals are unable remember the event in a way that gives it meaning and context. A rape victim who cannot coherently remember the event may remember only bits and pieces (e.g., the attacker repeatedly telling her she is stupid); because she was unable to develop a fully integrated memory, the fragmentary memory tends to stand out. Although unable to retrieve a complete memory of the event, she may be haunted by intrusive fragments involuntarily triggered by stimuli associated with the event (e.g., memories of the attacker’s comments when encountering a person who resembles the attacker). This interpretation fits previously discussed material concerning PTSD and conditioning. The model also proposes that negative appraisals of the event (“I deserved to be raped because I’m stupid”) may lead to dysfunctional behavioral strategies (e.g., avoiding social activities where men are likely to be present) that maintain PTSD symptoms by preventing both a change in the nature of the memory and a change in the problematic appraisals.
Try It
Mood and Related Disorders
 Mood disorders are those in which the person experiences severe disturbances in mood and emotion. They include depressive disorders and bipolar and related disorders. Depressive disorders include major depressive disorder, which is characterized by episodes of profound sadness and loss of interest or pleasure in usual activities and other associated features, and persistent depressive disorder, which marked by a chronic state of sadness. Bipolar disorder is characterized by mood states that vacillate between sadness and euphoria; a diagnosis of bipolar disorder requires experiencing at least one manic episode, which is defined as a period of extreme euphoria, irritability, and increased activity.
Mood disorders are those in which the person experiences severe disturbances in mood and emotion. They include depressive disorders and bipolar and related disorders. Depressive disorders include major depressive disorder, which is characterized by episodes of profound sadness and loss of interest or pleasure in usual activities and other associated features, and persistent depressive disorder, which marked by a chronic state of sadness. Bipolar disorder is characterized by mood states that vacillate between sadness and euphoria; a diagnosis of bipolar disorder requires experiencing at least one manic episode, which is defined as a period of extreme euphoria, irritability, and increased activity.
Mood disorders appear to have a genetic component, with genetic factors playing a more prominent role in bipolar disorder than in depression. Both biological and psychological factors are important in the development of depression. People who suffer from mental health problems, especially mood disorders, are at heightened risk for suicide.
Mood and Related Disorders
Learning Objectives
- Describe the symptoms, results, and risk factors of major depressive disorder
- Understand the differences between major depressive disorder and persistent depressive disorder, and identify two subtypes of depression
- Describe the symptoms and risk factors of bipolar disorder
- Describe genetic, biological, and psychological explanations of major depressive disorder
- Discuss the relationship between mood disorders and suicidal ideation, as well as factors associated with suicide
Major Depressive Disorder
Blake cries all day and feeling that he is worthless and his life is hopeless, he cannot get out of bed. Crystal stays up all night, talks very rapidly, and went on a shopping spree in which she spent $3,000 on furniture, although she cannot afford it. Maria recently had a baby, and she feels overwhelmed, teary, anxious, and panicked, and believes she is a terrible mother—practically every day since the baby was born. All these individuals demonstrate symptoms of a potential mood disorder.
Mood disorders (Figure 15) are characterized by severe disturbances in mood and emotions—most often depression, but also mania and elation (Rothschild, 1999). All of us experience fluctuations in our moods and emotional states, and often these fluctuations are caused by events in our lives. We become elated if our favorite team wins the World Series and dejected if a romantic relationship ends or if we lose our job. At times, we feel fantastic or miserable for no clear reason. People with mood disorders also experience mood fluctuations, but their fluctuations are extreme, distort their outlook on life, and impair their ability to function.

The DSM-5 lists two general categories of mood disorders. Depressive disorders are a group of disorders in which depression is the main feature. Depression is a vague term that, in everyday language, refers to an intense and persistent sadness. Depression is a heterogeneous mood state—it consists of a broad spectrum of symptoms that range in severity. Depressed people feel sad, discouraged, and hopeless. These individuals lose interest in activities once enjoyed, often experience a decrease in drives such as hunger and sex, and frequently doubt personal worth. Depressive disorders vary by degree, but this module highlights the most well-known: major depressive disorder (sometimes called unipolar depression).
Bipolar and related disorders are a group of disorders in which mania is the defining feature. Mania is a state of extreme elation and agitation. When people experience mania, they may become extremely talkative, behave recklessly, or attempt to take on many tasks simultaneously. The most recognized of these disorders is bipolar disorder.
What is Major Depressive Disorder?
According to the DSM-5, the defining symptoms of major depressive disorder include “depressed mood most of the day, nearly every day” (feeling sad, empty, hopeless, or appearing tearful to others), and loss of interest and pleasure in usual activities (APA, 2013). In addition to feeling overwhelmingly sad most of each day, people with depression will no longer show interest or enjoyment in activities that previously were gratifying, such as hobbies, sports, sex, social events, time spent with family, and so on. Friends and family members may notice that the person has completely abandoned previously enjoyed hobbies; for example, an avid tennis player who develops major depressive disorder no longer plays tennis (Rothschild, 1999).
To receive a diagnosis of major depressive disorder, one must experience a total of five symptoms for at least a two-week period; these symptoms must cause significant distress or impair normal functioning, and they must not be caused by substances or a medical condition. At least one of the two symptoms mentioned above must be present, plus any combination of the following symptoms (APA, 2013):
- significant weight loss (when not dieting) or weight gain and/or significant decrease or increase in appetite;
- difficulty falling asleep or sleeping too much;
- psychomotor agitation (the person is noticeably fidgety and jittery, demonstrated by behaviors like the inability to sit, pacing, hand-wringing, pulling or rubbing of the skin, clothing, or other objects) or psychomotor retardation (the person talks and moves slowly, for example, talking softly, very little, or in a monotone);
- fatigue or loss of energy;
- feelings of worthlessness or guilt;
- difficulty concentrating and indecisiveness; and
- suicidal ideation: thoughts of death (not just fear of dying), thinking about or planning suicide, or making an actual suicide attempt.
Major depressive disorder is considered episodic: its symptoms are typically present at their full magnitude for a certain period of time and then gradually abate. Approximately 50%–60% of people who experience an episode of major depressive disorder will have a second episode at some point in the future; those who have had two episodes have a 70% chance of having a third episode, and those who have had three episodes have a 90% chance of having a fourth episode (Rothschild, 1999). Although the episodes can last for months, a majority a people diagnosed with this condition (around 70%) recover within a year. However, a substantial number do not recover; around 12% show serious signs of impairment associated with major depressive disorder after 5 years (Boland & Keller, 2009). In the long-term, many who do recover will still show minor symptoms that fluctuate in their severity (Judd, 2012).
Try It
Results of Major Depressive Disorder
Major depressive disorder is a serious and incapacitating condition that can have a devastating effect on the quality of one’s life. The person suffering from this disorder lives a profoundly miserable existence that often results in unavailability for work or education, abandonment of promising careers, and lost wages; occasionally, the condition requires hospitalization. The majority of those with major depressive disorder report having faced some kind of discrimination, and many report that having received such treatment has stopped them from initiating close relationships, applying for jobs for which they are qualified, and applying for education or training (Lasalvia et al., 2013). Major depressive disorder also takes a toll on health. Depression is a risk factor for the development of heart disease in healthy patients, as well as adverse cardiovascular outcomes in patients with preexisting heart disease (Whooley, 2006).
Risk Factors for Major Depressive Disorder
Major depressive disorder is often referred to as the common cold of psychiatric disorders. Around 6.6% of the U.S. population experiences major depressive disorder each year; 16.9% will experience the disorder during their lifetime (Kessler & Wang, 2009). It is more common among women than among men, affecting approximately 20% of women and 13% of men at some point in their life (National Comorbidity Survey, 2007). The greater risk among women is not accounted for by a tendency to report symptoms or to seek help more readily, suggesting that gender differences in the rates of major depressive disorder may reflect biological and gender-related environmental experiences (Kessler, 2003).
Lifetime rates of major depressive disorder tend to be highest in North and South America, Europe, and Australia; they are considerably lower in Asian countries (Hasin, Fenton, & Weissman, 2011). The rates of major depressive disorder are higher among younger age cohorts than among older cohorts, perhaps because people in younger age cohorts are more willing to admit depression (Kessler & Wang, 2009).
A number of risk factors are associated with major depressive disorder: unemployment (including homemakers); earning less than $20,000 per year; living in urban areas; or being separated, divorced, or widowed (Hasin et al., 2011). Comorbid disorders include anxiety disorders and substance abuse disorders (Kessler & Wang, 2009).
Try It
Subtypes of Depression
The DSM-5 lists several different subtypes of depression. These subtypes—what the DSM-5 refer to as specifiers—are not specific disorders; rather, they are labels used to indicate specific patterns of symptoms or to specify certain periods of time in which the symptoms may be present. One subtype, seasonal pattern, applies to situations in which a person experiences the symptoms of major depressive disorder only during a particular time of year (e.g., fall or winter). In everyday language, people often refer to this subtype as the winter blues.
Another subtype, peripartum onset (commonly referred to as postpartum depression), applies to women who experience major depression during pregnancy or in the four weeks following the birth of their child (APA, 2013). These women often feel very anxious and may even have panic attacks. They may feel guilty, agitated, and be weepy. They may not want to hold or care for their newborn, even in cases in which the pregnancy was desired and intended. In extreme cases, the mother may have feelings of wanting to harm her child or herself. In a horrific illustration, a woman named Andrea Yates, who suffered from extreme peripartum-onset depression (as well as other mental illnesses), drowned her five children in a bathtub (Roche, 2002). Most women with peripartum-onset depression do not physically harm their children, but most do have difficulty being adequate caregivers (Fields, 2010). A surprisingly high number of women experience symptoms of peripartum-onset depression. A study of 10,000 women who had recently given birth found that 14% screened positive for peripartum-onset depression, and that nearly 20% reported having thoughts of wanting to harm themselves (Wisner et al., 2013).
People with persistent depressive disorder (previously known as dysthymia) experience depressed moods most of the day nearly every day for at least two years, as well as at least two of the other symptoms of major depressive disorder. People with persistent depressive disorder are chronically sad and melancholy, but do not meet all the criteria for major depression. However, episodes of full-blown major depressive disorder can occur during persistent depressive disorder (APA, 2013).
Try It
Bipolar Disorder
A person with bipolar disorder (commonly known as manic depression) often experiences mood states that vacillate between depression and mania; that is, the person’s mood is said to alternate from one emotional extreme to the other (in contrast to unipolar, which indicates a persistently sad mood).
To be diagnosed with bipolar disorder, a person must have experienced a manic episode at least once in his life; although major depressive episodes are common in bipolar disorder, they are not required for a diagnosis (APA, 2013). According to the DSM-5, a manic episode is characterized as a “distinct period of abnormally and persistently elevated, expansive, or irritable mood and abnormally and persistently increased activity or energy lasting at least one week,” that lasts most of the time each day (APA, 2013, p. 124). During a manic episode, some experience a mood that is almost euphoric and become excessively talkative, sometimes spontaneously starting conversations with strangers; others become excessively irritable and complain or make hostile comments. The person may talk loudly and rapidly, exhibiting flight of ideas, abruptly switching from one topic to another. These individuals are easily distracted, which can make a conversation very difficult. They may exhibit grandiosity, in which they experience inflated but unjustified self-esteem and self-confidence. For example, they might quit a job in order to “strike it rich” in the stock market, despite lacking the knowledge, experience, and capital for such an endeavor. They may take on several tasks at the same time (e.g., several time-consuming projects at work) and yet show little, if any, need for sleep; some may go for days without sleep. Patients may also recklessly engage in pleasurable activities that could have harmful consequences, including spending sprees, reckless driving, making foolish investments, excessive gambling, or engaging in sexual encounters with strangers (APA, 2013).
During a manic episode, individuals usually feel as though they are not ill and do not need treatment. However, the reckless behaviors that often accompany these episodes—which can be antisocial, illegal, or physically threatening to others—may require involuntary hospitalization (APA, 2013). Some patients with bipolar disorder will experience a rapid-cycling subtype, which is characterized by at least four manic episodes (or some combination of at least four manic and major depressive episodes) within one year.
Watch It
Not sleeping for days on end. Long periods of euphoria. Racing thoughts. Grandiose ideas. Mania. Depression. All of these are symptoms of Bipolar Disorder. In the following episode of Crash Course Psychology, Hank talks about mood disorders and their causes as well as how these disorders can impact people’s lives.
Risk Factors for Bipolar Disorder
Bipolar disorder is considerably less frequent than major depressive disorder. In the United States, 1 out of every 167 people meets the criteria for bipolar disorder each year, and 1 out of 100 meet the criteria within their lifetime (Merikangas et al., 2011). The rates are higher in men than in women, and about half of those with this disorder report onset before the age of 25 (Merikangas et al., 2011). Around 90% of those with bipolar disorder have a comorbid disorder, most often an anxiety disorder or a substance abuse problem. Unfortunately, close to half of the people suffering from bipolar disorder do not receive treatment (Merikangas & Tohen, 2011). Suicide rates are extremely high among those with bipolar disorder: around 36% of individuals with this disorder attempt suicide at least once in their lifetime (Novick, Swartz, & Frank, 2010), and between 15%–19% complete suicide (Newman, 2004).
Try It
The Biological Basis of Mood Disorders

Depression is linked to abnormal activity in several regions of the brain (Fitzgerald, Laird, Maller, & Daskalakis, 2008) including those important in assessing the emotional significance of stimuli and experiencing emotions (amygdala), and in regulating and controlling emotions (like the prefrontal cortex, or PFC) (LeMoult, Castonguay, Joormann, & McAleavey, 2013). Depressed individuals show elevated amygdala activity (Drevets, Bogers, & Raichle, 2002), especially when presented with negative emotional stimuli, such as photos of sad faces (Figure 17) (Surguladze et al., 2005). Interestingly, heightened amygdala activation to negative emotional stimuli among depressed persons occurs even when stimuli are presented outside of conscious awareness (Victor, Furey, Fromm, Öhman, & Drevets, 2010), and it persists even after the negative emotional stimuli are no longer present (Siegle, Thompson, Carter, Steinhauer, & Thase, 2007). Additionally, depressed individuals exhibit less activation in the prefrontal, particularly on the left side (Davidson, Pizzagalli, & Nitschke, 2009). Because the PFC can dampen amygdala activation, thereby enabling one to suppress negative emotions (Phan et al., 2005), decreased activation in certain regions of the PFC may inhibit its ability to override negative emotions that might then lead to more negative mood states (Davidson et al., 2009). These findings suggest that depressed persons are more prone to react to emotionally negative stimuli, yet have greater difficulty controlling these reactions.

Since the 1950s, researchers have noted that depressed individuals have abnormal levels of cortisol, a stress hormone released into the blood by the neuroendocrine system during times of stress (Mackin & Young, 2004). When cortisol is released, the body initiates a fight-or-flight response in reaction to a threat or danger. Many people with depression show elevated cortisol levels (Holsboer & Ising, 2010), especially those reporting a history of early life trauma such as the loss of a parent or abuse during childhood (Baes, Tofoli, Martins, & Juruena, 2012). Such findings raise the question of whether high cortisol levels are a cause or a consequence of depression. High levels of cortisol are a risk factor for future depression (Halligan, Herbert, Goodyer, & Murray, 2007), and cortisol activates activity in the amygdala while deactivating activity in the PFC (McEwen, 2005)—both brain disturbances are connected to depression. Thus, high cortisol levels may have a causal effect on depression, as well as on its brain function abnormalities (van Praag, 2005). Also, because stress results in increased cortisol release (Michaud, Matheson, Kelly, Anisman, 2008), it is equally reasonable to assume that stress may precipitate depression.
Diathesis-Stress Model and Major Depressive Disorders
Indeed, it has long been believed that stressful life events can trigger depression, and research has consistently supported this conclusion (Mazure, 1998). Stressful life events include significant losses, such as death of a loved one, divorce or separation, and serious health and money problems; life events such as these often precede the onset of depressive episodes (Brown & Harris, 1989). In particular, exit events—instances in which an important person departs (e.g., a death, divorce or separation, or a family member leaving home)—often occur prior to an episode (Paykel, 2003). Exit events are especially likely to trigger depression if these happenings occur in a way that humiliates or devalues the individual. For example, people who experience the breakup of a relationship initiated by the other person develop major depressive disorder at a rate more than 2 times that of people who experience the death of a loved one (Kendler, Hettema, Butera, Gardner, & Prescott, 2003).
Likewise, individuals who are exposed to traumatic stress during childhood—such as separation from a parent, family turmoil, and maltreatment (physical or sexual abuse)—are at a heightened risk of developing depression at any point in their lives (Kessler, 1997). A recent review of 16 studies involving over 23,000 subjects concluded that those who experience childhood maltreatment are more than 2 times as likely to develop recurring and persistent depression (Nanni, Uher, & Danese, 2012).
Of course, not everyone who experiences stressful life events or childhood adversities succumbs to depression—indeed, most do not. Clearly, a diathesis-stress interpretation of major depressive disorder, in which certain predispositions or vulnerability factors influence one’s reaction to stress, would seem logical. If so, what might such predispositions be? A study by Caspi and others (2003) suggests that an alteration in a specific gene that regulates serotonin (the 5-HTTLPR gene) might be one culprit. These investigators found that people who experienced several stressful life events were significantly more likely to experience episodes of major depression if they carried one or two short versions of this gene than if they carried two long versions. Those who carried one or two short versions of the 5-HTTLPR gene were unlikely to experience an episode, however, if they had experienced few or no stressful life events. Numerous studies have replicated these findings, including studies of people who experienced maltreatment during childhood (Goodman & Brand, 2009). In a recent investigation conducted in the United Kingdom (Brown & Harris, 2013), researchers found that childhood maltreatment before age 9 elevated the risk of chronic adult depression (a depression episode lasting for at least 12 months) among those individuals having one (LS) or two (SS) short versions of the 5-HTTLPR gene (Figure 18). Childhood maltreatment did not increase the risk for chronic depression for those have two long (LL) versions of this gene. Thus, genetic vulnerability may be one mechanism through which stress potentially leads to depression.

Cognitive Theories of Depression
Cognitive theories of depression take the view that depression is triggered by negative thoughts, interpretations, self-evaluations, and expectations (Joormann, 2009). These diathesis-stress models propose that depression is triggered by a “cognitive vulnerability” (negative and maladaptive thinking) and by precipitating stressful life events (Gotlib & Joormann, 2010). Perhaps the most well-known cognitive theory of depression was developed in the 1960s by psychiatrist Aaron Beck, based on clinical observations and supported by research (Beck, 2008). Beck theorized that depression-prone people possess depressive schemas, or mental predispositions to think about most things in a negative way (Beck, 1976). Depressive schemas contain themes of loss, failure, rejection, worthlessness, and inadequacy, and may develop early in childhood in response to adverse experiences, then remain dormant until they are activated by stressful or negative life events. Depressive schemas prompt dysfunctional and pessimistic thoughts about the self, the world, and the future. Beck believed that this dysfunctional style of thinking is maintained by cognitive biases, or errors in how we process information about ourselves, which lead us to focus on negative aspects of experiences, interpret things negatively, and block positive memories (Beck, 2008). A person whose depressive schema consists of a theme of rejection might be overly attentive to social cues of rejection (more likely to notice another’s frown), and he might interpret this cue as a sign of rejection and automatically remember past incidents of rejection. Longitudinal studies have supported Beck’s theory, in showing that a preexisting tendency to engage in this negative, self-defeating style of thinking—when combined with life stress—over time predicts the onset of depression (Dozois & Beck, 2008). Cognitive therapies for depression, aimed at changing a depressed person’s negative thinking, were developed as an expansion of this theory (Beck, 1976).
Another cognitive theory of depression, hopelessness theory, postulates that a particular style of negative thinking leads to a sense of hopelessness, which then leads to depression (Abramson, Metalsky, & Alloy, 1989). According to this theory, hopelessness is an expectation that unpleasant outcomes will occur or that desired outcomes will not occur, and there is nothing one can do to prevent such outcomes. A key assumption of this theory is that hopelessness stems from a tendency to perceive negative life events as having stable (“It’s never going to change”) and global (“It’s going to affect my whole life”) causes, in contrast to unstable (“It’s fixable”) and specific (“It applies only to this particular situation”) causes, especially if these negative life events occur in important life realms, such as relationships, academic achievement, and the like. Suppose a student who wishes to go to law school does poorly on an admissions test. If the student infers negative life events as having stable and global causes, she may believe that her poor performance has a stable and global cause (“I lack intelligence, and it’s going to prevent me from ever finding a meaningful career”), as opposed to an unstable and specific cause (“I was sick the day of the exam, so my low score was a fluke”). Hopelessness theory predicts that people who exhibit this cognitive style in response to undesirable life events will view such events as having negative implications for their future and self-worth, thereby increasing the likelihood of hopelessness—the primary cause of depression (Abramson et al., 1989). One study testing hopelessness theory measured the tendency to make negative inferences for bad life effects in participants who were experiencing uncontrollable stressors. Over the ensuing six months, those with scores reflecting high cognitive vulnerability were 7 times more likely to develop depression compared to those with lower scores (Kleim, Gonzalo, & Ehlers, 2011).
A third cognitive theory of depression focuses on how people’s thoughts about their distressed moods—depressed symptoms in particular—can increase the risk and duration of depression. This theory, which focuses on rumination in the development of depression, was first described in the late 1980s to explain the higher rates of depression in women than in men (Nolen-Hoeksema, 1987). Rumination is the repetitive and passive focus on the fact that one is depressed and dwelling on depressed symptoms, rather that distracting one’s self from the symptoms or attempting to address them in an active, problem-solving manner (Nolen-Hoeksema, 1991). When people ruminate, they have thoughts such as “Why am I so unmotivated? I just can’t get going. I’m never going to get my work done feeling this way” (Nolen-Hoeksema & Hilt, 2009, p. 393). Women are more likely than men to ruminate when they are sad or depressed (Butler & Nolen-Hoeksema, 1994), and the tendency to ruminate is associated with increases in depression symptoms (Nolen-Hoeksema, Larson, & Grayson, 1999), heightened risk of major depressive episodes (Abela & Hankin, 2011), and chronicity of such episodes (Robinson & Alloy, 2003).
Try It
Schizophrenia and Dissociative Disorders

Schizophrenia is a severe disorder characterized by a complete breakdown in one’s ability to function in life; it often requires hospitalization. People with schizophrenia experience hallucinations and delusions, and they have extreme difficulty regulating their emotions and behavior. Thinking is incoherent and disorganized, behavior is extremely bizarre, emotions are flat, and motivation to engage in most basic life activities is lacking.
Schizophrenia is not to be confused with multiple personality disorder, which is technically termed dissociative identity disorder. The main characteristic of dissociative disorders is that people become dissociated from their sense of self, resulting in memory and identity disturbances. Dissociative disorders listed in the DSM-5 include dissociative amnesia, depersonalization/derealization disorder, and dissociative identity disorder. A person with dissociative amnesia is unable to recall important personal information, often after a stressful or traumatic experience. In this section, you’ll learn about the differences between schizophrenia and these disorders.
Schizophrenia and Dissociative Disorders
Learning Objectives
- Categorize and describe the major symptoms of schizophrenia
- Describe the interplay between genetic, biological, and environmental factors that are associated with the development of schizophrenia
- Identify and differentiate the symptoms and potential causes of dissociative amnesia, depersonalization/ derealization disorder, and dissociative identity disorder
Schizophrenia
Schizophrenia is a devastating psychological disorder that is characterized by major disturbances in thought, perception, emotion, and behavior. About 1% of the population experiences schizophrenia in their lifetime, and usually the disorder is first diagnosed during early adulthood (early to mid-20s). Most people with schizophrenia experience significant difficulties in many day-to-day activities, such as holding a job, paying bills, caring for oneself (grooming and hygiene), and maintaining relationships with others. Frequent hospitalizations are more often the rule rather than the exception with schizophrenia. Even when they receive the best treatments available, many with schizophrenia will continue to experience serious social and occupational impairment throughout their lives.
What is schizophrenia? First, schizophrenia is not a condition involving a split personality; that is, schizophrenia is not the same thing as dissociative identity disorder (better known as multiple personality disorder). These disorders are sometimes confused because the word schizophrenia first coined by the Swiss psychiatrist Eugen Bleuler in 1911, derives from Greek words that refer to a “splitting” (schizo) of psychic functions (phrene) (Green, 2001).
Schizophrenia is considered a psychotic disorder, or one in which the person’s thoughts, perceptions, and behaviors are impaired to the point where she is not able to function normally in life. In informal terms, one who suffers from a psychotic disorder (that is, has a psychosis) is disconnected from the world in which most of us live.
Symptoms of Schizophrenia
The main symptoms of schizophrenia include hallucinations, delusions, disorganized thinking, disorganized or abnormal motor behavior, and negative symptoms (APA, 2013). A hallucination is a perceptual experience that occurs in the absence of external stimulation. Auditory hallucinations (hearing voices) occur in roughly two-thirds of patients with schizophrenia and are by far the most common form of hallucination (Andreasen, 1987). The voices may be familiar or unfamiliar, they may have a conversation or argue, or the voices may provide a running commentary on the person’s behavior (Tsuang, Farone, & Green, 1999).
Less common are visual hallucinations (seeing things that are not there) and olfactory hallucinations (smelling odors that are not actually present).
Delusions are beliefs that are contrary to reality and are firmly held even in the face of contradictory evidence. Many of us hold beliefs that some would consider odd, but a delusion is easily identified because it is clearly absurd. A person with schizophrenia may believe that his mother is plotting with the FBI to poison his coffee, or that his neighbor is an enemy spy who wants to kill him. These kinds of delusions are known as paranoid delusions, which involve the (false) belief that other people or agencies are plotting to harm the person. People with schizophrenia also may hold grandiose delusions, beliefs that one holds special power, unique knowledge, or is extremely important. For example, the person who claims to be Jesus Christ, or who claims to have knowledge going back 5,000 years, or who claims to be a great philosopher is experiencing grandiose delusions. Other delusions include the belief that one’s thoughts are being removed (thought withdrawal) or thoughts have been placed inside one’s head (thought insertion). Another type of delusion is somatic delusion, which is the belief that something highly abnormal is happening to one’s body (e.g., that one’s kidneys are being eaten by cockroaches).
Disorganized thinking refers to disjointed and incoherent thought processes—usually detected by what a person says. The person might ramble, exhibit loose associations (jump from topic to topic), or talk in a way that is so disorganized and incomprehensible that it seems as though the person is randomly combining words. Disorganized thinking is also exhibited by blatantly illogical remarks (e.g., “Fenway Park is in Boston. I live in Boston. Therefore, I live at Fenway Park.”) and by tangentiality: responding to others’ statements or questions by remarks that are either barely related or unrelated to what was said or asked. For example, if a person diagnosed with schizophrenia is asked if she is interested in receiving special job training, she might state that she once rode on a train somewhere. To a person with schizophrenia, the tangential (slightly related) connection between job training and riding a train are sufficient enough to cause such a response.
Disorganized or abnormal motor behavior refers to unusual behaviors and movements: becoming unusually active, exhibiting silly child-like behaviors (giggling and self-absorbed smiling), engaging in repeated and purposeless movements, or displaying odd facial expressions and gestures. In some cases, the person will exhibit catatonic behaviors, which show decreased reactivity to the environment, such as posturing, in which the person maintains a rigid and bizarre posture for long periods of time, or catatonic stupor, a complete lack of movement and verbal behavior.
Schizophrenia has positive and negative symptoms. Positive symptoms of schizophrenia are symptoms of commission, meaning they are something that individuals do or think. Examples include the hallucinations, delusions, and bizarre or disorganized behavior describe above. Negative symptoms are those that reflect noticeable decreases and absences in certain behaviors, emotions, or drives (Green, 2001). A person who exhibits diminished emotional expression shows no emotion in his facial expressions, speech, or movements, even when such expressions are normal or expected (also known as flat affect). Avolition is characterized by a lack of motivation to engage in self-initiated and meaningful activity, including the most basic of tasks, such as bathing and grooming. Alogia refers to reduced speech output; in simple terms, patients do not say much. Another negative symptom is asociality, or social withdrawal and lack of interest in engaging in social interactions with others. A final negative symptom, anhedonia, refers to an inability to experience pleasure. One who exhibits anhedonia expresses little interest in what most people consider to be pleasurable activities, such as hobbies, recreation, or sexual activity.
Link to Learning
Try It
Causes of Schizophrenia
Genes
When considering the role of genetics in schizophrenia, as in any disorder, conclusions based on family and twin studies are subject to criticism. This is because family members who are closely related (such as siblings) are more likely to share similar environments than are family members who are less closely related (such as cousins); further, identical twins may be more likely to be treated similarly by others than might fraternal twins. Thus, family and twin studies cannot completely rule out the possible effects of shared environments and experiences. Such problems can be corrected by using adoption studies, in which children are separated from their parents at an early age. One of the first adoption studies of schizophrenia conducted by Heston (1966) followed 97 adoptees, including 47 who were born to mothers with schizophrenia, over a 36-year period. Five of the 47 adoptees (11%) whose mothers had schizophrenia were later diagnosed with schizophrenia, compared to none of the 50 control adoptees. Other adoption studies have consistently reported that for adoptees who are later diagnosed with schizophrenia, their biological relatives have a higher risk of schizophrenia than do adoptive relatives (Shih, Belmonte, & Zandi, 2004).
Although adoption studies have supported the hypothesis that genetic factors contribute to schizophrenia, they have also demonstrated that the disorder most likely arises from a combination of genetic and environmental factors, rather than just genes themselves. For example, investigators in one study examined the rates of schizophrenia among 303 adoptees (Tienari et al., 2004). A total of 145 of the adoptees had biological mothers with schizophrenia; these adoptees constituted the high genetic risk group. The other 158 adoptees had mothers with no psychiatric history; these adoptees composed the low genetic risk group. The researchers managed to determine whether the adoptees’ families were either healthy or disturbed. For example, the adoptees were considered to be raised in a disturbed family environment if the family exhibited a lot of criticism, conflict, and a lack of problem-solving skills. The findings revealed that adoptees whose mothers had schizophrenia (high genetic risk) and who had been raised in a disturbed family environment were much more likely to develop schizophrenia or another psychotic disorder (36.8%) than were adoptees whose biological mothers had schizophrenia but who had been raised in a healthy environment (5.8%), or than adoptees with a low genetic risk who were raised in either a disturbed (5.3%) or healthy (4.8%) environment. Because the adoptees who were at high genetic risk were likely to develop schizophrenia only if they were raised in a disturbed home environment, this study supports a diathesis-stress interpretation of schizophrenia—both genetic vulnerability and environmental stress are necessary for schizophrenia to develop, genes alone do not show the complete picture.
Neurotransmitters
If we accept that schizophrenia is at least partly genetic in origin, as it seems to be, it makes sense that the next step should be to identify biological abnormalities commonly found in people with the disorder. Perhaps not surprisingly, a number of neurobiological factors have indeed been found to be related to schizophrenia. One such factor that has received considerable attention for many years is the neurotransmitter dopamine. Interest in the role of dopamine in schizophrenia was stimulated by two sets of findings: drugs that increase dopamine levels can produce schizophrenia-like symptoms, and medications that block dopamine activity reduce the symptoms (Howes & Kapur, 2009). The dopamine hypothesis of schizophrenia proposed that an overabundance of dopamine or too many dopamine receptors are responsible for the onset and maintenance of schizophrenia (Snyder, 1976). More recent work in this area suggests that abnormalities in dopamine vary by brain region and thus contribute to symptoms in unique ways. In general, this research has suggested that an overabundance of dopamine in the limbic system may be responsible for some symptoms, such as hallucinations and delusions, whereas low levels of dopamine in the prefrontal cortex might be responsible primarily for the negative symptoms (avolition, alogia, asociality, and anhedonia) (Davis, Kahn, Ko, & Davidson, 1991). In recent years, serotonin has received attention, and newer antipsychotic medications used to treat the disorder work by blocking serotonin receptors (Baumeister & Hawkins, 2004).
Brain Anatomy
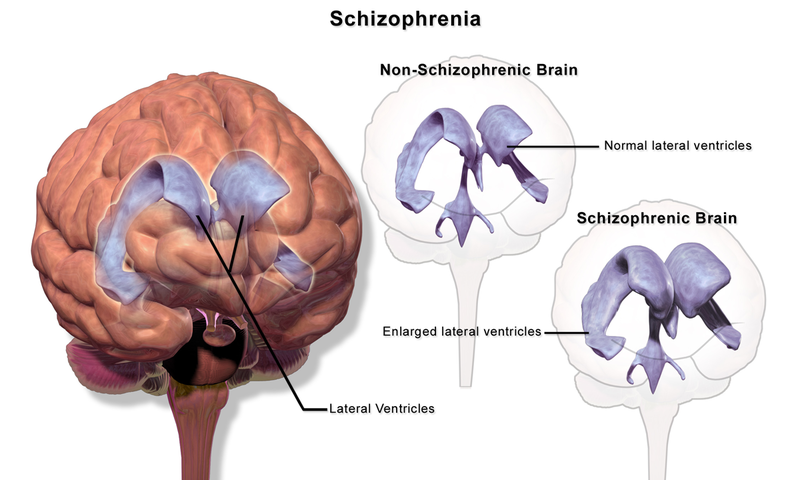
Brain imaging studies reveal that people with schizophrenia have enlarged ventricles, the cavities within the brain that contain cerebral spinal fluid (Green, 2001). This finding is important because larger than normal ventricles suggests that various brain regions are reduced in size, thus implying that schizophrenia is associated with a loss of brain tissue. In addition, many people with schizophrenia display a reduction in gray matter (cell bodies of neurons) in the frontal lobes (Lawrie & Abukmeil, 1998), and many show less frontal lobe activity when performing cognitive tasks (Buchsbaum et al., 1990). The frontal lobes are important in a variety of complex cognitive functions, such as planning and executing behavior, attention, speech, movement, and problem solving. Hence, abnormalities in this region provide merit in explaining why people with schizophrenia experience deficits in these of areas.
Events During Pregnancy
Why do people with schizophrenia have these brain abnormalities? A number of environmental factors that could impact normal brain development might be at fault. High rates of obstetric complications in the births of children who later developed schizophrenia have been reported (Cannon, Jones, & Murray, 2002). In addition, people are at an increased risk for developing schizophrenia if their mother was exposed to influenza during the first trimester of pregnancy (Brown et al., 2004). Research has also suggested that a mother’s emotional stress during pregnancy may increase the risk of schizophrenia in offspring. One study reported that the risk of schizophrenia is elevated substantially in offspring whose mothers experienced the death of a relative during the first trimester of pregnancy (Khashan et al., 2008).
Marijuana
Another variable that is linked to schizophrenia is marijuana use. Although a number of reports have shown that individuals with schizophrenia are more likely to use marijuana than are individuals without schizophrenia (Thornicroft, 1990), such investigations cannot determine if marijuana use leads to schizophrenia, or vice versa. However, a number of longitudinal studies have suggested that marijuana use is, in fact, a risk factor for schizophrenia. A classic investigation of over 45,000 Swedish conscripts who were followed up after 15 years found that those individuals who had reported using marijuana at least once by the time of conscription were more than 2 times as likely to develop schizophrenia during the ensuing 15 years than were those who reported never using marijuana; those who had indicated using marijuana 50 or more times were 6 times as likely to develop schizophrenia (Andréasson, Allbeck, Engström, & Rydberg, 1987). More recently, a review of 35 longitudinal studies found a substantially increased risk of schizophrenia and other psychotic disorders in people who had used marijuana, with the greatest risk in the most frequent users (Moore et al., 2007). Other work has found that marijuana use is associated with an onset of psychotic disorders at an earlier age (Large, Sharma, Compton, Slade, & Nielssen, 2011). Overall, the available evidence seems to indicate that marijuana use plays a causal role in the development of schizophrenia, although it is important to point out that marijuana use is not an essential or sufficient risk factor as not all people with schizophrenia have used marijuana and the majority of marijuana users do not develop schizophrenia (Casadio, Fernandes, Murray, & Di Forti, 2011). One plausible interpretation of the data is that early marijuana use may disrupt normal brain development during important early maturation periods in adolescence (Trezza, Cuomo, & Vanderschuren, 2008). Thus, early marijuana use may set the stage for the development of schizophrenia and other psychotic disorders, especially among individuals with an established vulnerability (Casadio et al., 2011).
Schizophrenia: Early Warning Signs
Early detection and treatment of conditions such as heart disease and cancer have improved survival rates and quality of life for people who suffer from these conditions. A new approach involves identifying people who show minor symptoms of psychosis, such as unusual thought content, paranoia, odd communication, delusions, problems at school or work, and a decline in social functioning—which are coined prodromal symptoms—and following these individuals over time to determine which of them develop a psychotic disorder and which factors best predict such a disorder. A number of factors have been identified that predict a greater likelihood that prodromal individuals will develop a psychotic disorder: genetic risk (a family history of psychosis), recent deterioration in functioning, high levels of unusual thought content, high levels of suspicion or paranoia, poor social functioning, and a history of substance abuse (Fusar-Poli et al., 2013). Further research will enable a more accurate prediction of those at greatest risk for developing schizophrenia, and thus to whom early intervention efforts should be directed.
Try It
Dissociative Disorders

Dissociative disorders are characterized by an individual becoming split off, or dissociated, from her core sense of self. Memory and identity become disturbed; these disturbances have a psychological rather than physical cause. Dissociative disorders listed in the DSM-5 include dissociative amnesia, depersonalization/derealization disorder, and dissociative identity disorder.
Dissociative Amnesia
Amnesia refers to the partial or total forgetting of some experience or event. An individual with dissociative amnesia is unable to recall important personal information, usually following an extremely stressful or traumatic experience such as combat, natural disasters, or being the victim of violence. The memory impairments are not caused by ordinary forgetting. Some individuals with dissociative amnesia will also experience dissociative fugue (from the word “to flee” in French), whereby they suddenly wander away from their home, experience confusion about their identity, and sometimes even adopt a new identity (Cardeña & Gleaves, 2006). Most fugue episodes last only a few hours or days, but some can last longer. One study of residents in communities in upstate New York reported that about 1.8% experienced dissociative amnesia in the previous year (Johnson, Cohen, Kasen, & Brook, 2006).
Some have questioned the validity of dissociative amnesia (Pope, Hudson, Bodkin, & Oliva, 1998); it has even been characterized as a “piece of psychiatric folklore devoid of convincing empirical support” (McNally, 2003, p. 275). Notably, scientific publications regarding dissociative amnesia rose during the 1980s and reached a peak in the mid-1990s, followed by an equally sharp decline by 2003; in fact, only 13 cases of individuals with dissociative amnesia worldwide could be found in the literature that same year (Pope, Barry, Bodkin, & Hudson, 2006). Further, no description of individuals showing dissociative amnesia following a trauma exists in any fictional or nonfictional work prior to 1800 (Pope, Poliakoff, Parker, Boynes, & Hudson, 2006). However, a study of 82 individuals who enrolled for treatment at a psychiatric outpatient hospital found that nearly 10% met the criteria for dissociative amnesia, perhaps suggesting that the condition is underdiagnosed, especially in psychiatric populations (Foote, Smolin, Kaplan, Legatt, & Lipschitz, 2006).
Try It
Depersonalization/Derealization Disorder
Depersonalization/derealization disorder is characterized by recurring episodes of depersonalization, derealization, or both. Depersonalization is defined as feelings of “unreality or detachment from, or unfamiliarity with, one’s whole self or from aspects of the self” (APA, 2013, p. 302). Individuals who experience depersonalization might believe their thoughts and feelings are not their own; they may feel robotic as though they lack control over their movements and speech; they may experience a distorted sense of time and, in extreme cases, they may sense an “out-of-body” experience in which they see themselves from the vantage point of another person. Derealization is conceptualized as a sense of “unreality or detachment from, or unfamiliarity with, the world, be it individuals, inanimate objects, or all surroundings” (APA, 2013, p. 303). A person who experiences derealization might feel as though he is in a fog or a dream, or that the surrounding world is somehow artificial and unreal. Individuals with depersonalization/derealization disorder often have difficulty describing their symptoms and may think they are going crazy (APA, 2013).
Dissociative Identity Disorder
By far, the most well-known dissociative disorder is dissociative identity disorder (formerly called multiple personality disorder). People with dissociative identity disorder exhibit two or more separate personalities or identities, each well-defined and distinct from one another. They also experience memory gaps for the time during which another identity is in charge (e.g., one might find unfamiliar items in her shopping bags or among her possessions), and in some cases may report hearing voices, such as a child’s voice or the sound of somebody crying (APA, 2013). The study of upstate New York residents mentioned above (Johnson et al., 2006) reported that 1.5% of their sample experienced symptoms consistent with dissociative identity disorder in the previous year.
Dissociative identity disorder (DID) is highly controversial. Some believe that people fake symptoms to avoid the consequences of illegal actions (e.g., “I am not responsible for shoplifting because it was my other personality”). In fact, it has been demonstrated that people are generally skilled at adopting the role of a person with different personalities when they believe it might be advantageous to do so. As an example, Kenneth Bianchi was an infamous serial killer who, along with his cousin, murdered over a dozen females around Los Angeles in the late 1970s. Eventually, he and his cousin were apprehended. At Bianchi’s trial, he pled not guilty by reason of insanity, presenting himself as though he had DID and claiming that a different personality (“Steve Walker”) committed the murders. When these claims were scrutinized, he admitted faking the symptoms and was found guilty (Schwartz, 1981).
A second reason DID is controversial is because rates of the disorder suddenly skyrocketed in the 1980s. More cases of DID were identified during the five years prior to 1986 than in the preceding two centuries (Putnam, Guroff, Silberman, Barban, & Post, 1986). Although this increase may be due to the development of more sophisticated diagnostic techniques, it is also possible that the popularization of DID—helped in part by Sybil, a popular 1970s book (and later film) about a woman with 16 different personalities—may have prompted clinicians to overdiagnose the disorder (Piper & Merskey, 2004). Casting further scrutiny on the existence of multiple personalities or identities is the recent suggestion that the story of Sybil was largely fabricated, and the idea for the book might have been exaggerated (Nathan, 2011).
Despite its controversial nature, DID is clearly a legitimate and serious disorder, and although some people may fake symptoms, others suffer their entire lives with it. People with this disorder tend to report a history of childhood trauma, some cases having been corroborated through medical or legal records (Cardeña & Gleaves, 2006). Research by Ross et al. (1990) suggests that in one study about 95% of people with DID were physically and/or sexually abused as children. Of course, not all reports of childhood abuse can be expected to be valid or accurate. However, there is strong evidence that traumatic experiences can cause people to experience states of dissociation, suggesting that dissociative states—including the adoption of multiple personalities—may serve as a psychologically important coping mechanism for threat and danger (Dalenberg et al., 2012).
Watch It
Review the differences between schizophrenia and the once-called multiple personality disorder in the following episode of CrashCourse Psychology.
Try It
Think It Over
- Try to find an example (via a search engine) of a past instance in which a person committed a horrible crime, was apprehended, and later claimed to have dissociative identity disorder during the trial. What was the outcome? Was the person revealed to be faking? If so, how was this determined?
Try It
Classifying Psychological Disorders
As you’ve learned, there are many different categories of mental disorders, and many different facets of human behavior and personality that can become disordered. Keep reading to review each of the main categorizations you learned about in this module.
Anxiety or fear that interferes with normal functioning may be classified as an anxiety disorder. Commonly recognized categories include specific phobias: a specific unrealistic fear; social anxiety disorder: extreme fear and avoidance of social situations; panic disorder: suddenly overwhelmed by panic even though there is no apparent reason to be frightened; agoraphobia: an intense fear and avoidance of situations in which it might be difficult to escape; and generalized anxiety disorder: a relatively continuous state of tension, apprehension, and dread. Posttraumatic stress disorder is similar disorder, although classified as a trauma- and stressor-related disorder.
Link to Learning
Learn more about each of the psychological disorders through the National Institute of Mental Health.
Or for an interesting application of the various mental disorders, take a look at this YouTube playlist with disorders as they are characterized in popular media. These case studies were developed by students in Dr. Caleb Lack’s psychology class.
While similar to anxiety disorders, obsessive compulsive disorders and posttraumatic stress disorders now have their own distinct categories of classification within the DSM-5 because symptoms of anxiety are not necessarily present. With obsessive-compulsive disorder, a person is obsessed with unwanted, unpleasant thoughts and/or compulsively engages in repetitive behaviors or mental acts, perhaps as a way of coping with the obsessions. PTSD is as a disorder in which the experience of a traumatic or profoundly stressful event, such as combat, sexual assault, or natural disaster, produces a constellation of symptoms that must last for one month or more. These symptoms include intrusive and distressing memories of the event, flashbacks, avoidance of stimuli or situations that are connected to the event, persistently negative emotional states, feeling detached from others, irritability, proneness toward outbursts, and a tendency to be easily startled.
Other affective (emotion/mood) processes can also become disordered. Mood disorder involving unusually intense and sustained sadness, melancholia, or despair is known as major depressive disorder. Milder but still prolonged depression can be diagnosed as dysthymia. Bipolar disorder is characterized by mood states that vacillate between sadness and euphoria; a diagnosis of bipolar disorder requires experiencing at least one manic episode, which is defined as a period of extreme euphoria, irritability, and increased activity. Mood disorders appear to have a genetic component, with genetic factors playing a more prominent role in bipolar disorder than in depression. Both biological and psychological factors are important in the development of depression. People who suffer from mental health problems, especially mood disorders, are at heightened risk for suicide.
Patterns of belief, language use and perception of reality can also become disordered (e.g., delusions, thought disorder, hallucinations). The most common psychotic disorder in this domain is schizophrenia, which is a severe disorder characterized by a complete breakdown in one’s ability to function in life. People with schizophrenia experience hallucinations and delusions, and they have extreme difficulty regulating their emotions and behavior. Thinking is incoherent and disorganized, behavior is extremely bizarre, emotions are flat, and motivation to engage in most basic life activities is lacking. Considerable evidence shows that genetic factors play a central role in schizophrenia; however, adoption studies have highlighted the additional importance of environmental factors. Neurotransmitter and brain abnormalities, which may be linked to environmental factors such as obstetric complications or exposure to influenza during the gestational period, have also been implicated. A promising new area of schizophrenia research involves identifying individuals who show prodromal symptoms and following them over time to determine which factors best predict the development of schizophrenia. Future research may enable us to pinpoint those especially at risk for developing schizophrenia and who may benefit from early intervention.
The main characteristic of dissociative disorders is that people become dissociated from their sense of self, resulting in memory and identity disturbances. Dissociative disorders listed in the DSM-5 include dissociative amnesia, depersonalization/derealization disorder, and dissociative identity disorder. A person with dissociative amnesia is unable to recall important personal information, often after a stressful or traumatic experience.
Depersonalization/derealization disorder is characterized by recurring episodes of depersonalization (i.e., detachment from or unfamiliarity with the self) and/or derealization (i.e., detachment from or unfamiliarity with the world). A person with dissociative identity disorder exhibits two or more well-defined and distinct personalities or identities, as well as memory gaps for the time during which another identity was present.
Dissociative identity disorder has generated controversy, mainly because some believe its symptoms can be faked by patients if presenting its symptoms somehow benefits the patient in avoiding negative consequences or taking responsibility for one’s actions. The diagnostic rates of this disorder have increased dramatically following its portrayal in popular culture. However, many people legitimately suffer over the course of a lifetime with this disorder.
Try It
Putting It Together: Psychological Disorders
Learning Objectives
In this chapter, you learned to
- define psychological disorders and explain how they are classified
- describe the features and characteristic symptoms of anxiety disorders (generalized anxiety disorder, panic disorder, phobias), obsessive-compulsive disorder and posttraumatic stress disorder; differentiate these anxiety disorders from each other
- describe the characteristic symptoms and risk factors of mood disorders, including major depressive disorder and bipolar disorder
- explain symptoms and potential causes of schizophrenic and dissociative disorders
This chapter covered a lot of ground and gave you a foundation for understanding psychological disorders. If you are interested in learning more, there are entire courses on abnormal psychology and classes on specific mental illnesses as well. In this module, you learned about how mental disorders are defined and classified using the DSM-V, and how psychologists, psychiatrists and other mental health professionals identify mental illnesses. One tendency while reading through this material is for students to self-diagnose, as it is easy to identify with various descriptions of mental disorders. Be wary of self-diagnosis as you may see symptoms that aren’t there, or miss symptoms or signs of something more serious. If you do think you may be suffering from a mental illness (defined as significant disturbances in thoughts, feelings, and behaviors causing impairment in one’s life), then please seek for help from a counselor, doctor, or other trained professional. Hopefully, reading this chapter has also helped you to better understand mental illness and be less inclined to judge or stigmatize those who are suffering from or managing an illness.
To quickly review the main disorders from your reading, take a moment to consider how you might visually or artistically represent each of the disorders.
Watch It
Watch this video from architect and graphic designer Federico Babina to see his interpretation of various mental disorders. How might you change or alter his depictions, or what would you add to this list?
Chapter References (Click to expand)
Abela, J. R., & Hankin, B. L. (2011). Rumination as a vulnerability factor to depression during the transition from early to middle adolescence: A multiwave longitudinal study. Journal of Abnormal Psychology, 120, 259–271.
Abramowitz, J. S., & Siqueland, L. (2013). Obsessive-compulsive disorder. In L. G. Castonguay & T. F. Oltmanns (Eds.), Psychopathology: From science to clinical practice (pp. 143–171). New York, NY: Guilford Press.
Abramson, L. Y., Metalsky, G. I., & Alloy, L. B. (1989). Hopelessness depression: A theory- based subtype of depression. Psychological Review, 96, 358–372.
Aghukwa, C. N. (2012). Care seeking and beliefs about the cause of mental illness among Nigerian psychiatric patients and their families. Psychiatric Services, 63, 616–618.
Aikins, D. E., & Craske, M. G. (2001). Cognitive theories of generalized anxiety disorder. Psychiatric Clinics of North America, 24, 57–74.
Alden, L. E., & Bieling, P. (1998). Interpersonal consequences in the pursuit of safety. Behaviour Research and Therapy, 36, 53–64.
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington, DC: Author.
Andreasen, N. C. (1987). The diagnosis of schizophrenia. Schizophrenia Bulletin, 13, 9–22.
Andréasson, S., Allbeck, P., Engström, A., & Rydberg, U. (1987). Cannabis and schizophrenia: A longitudinal study of Swedish conscripts. Lancet, 330, 1483–1486.
Baes, C. V. W., Tofoli, S. M. C., Martins, C. M. S., & Juruena, M. F. (2012). Assessment of the hypothalamic–pituitary–adrenal axis activity: Glucocorticoid receptor and mineralocorticoid receptor function in depression with early life stress—a systematic review. Acta Neuropsychiatrica, 24, 4–15.
Baker, L. A., Bezdjian, S., & Raine, A. (2006). Behavioral genetics: The science of antisocial behavior. Law and Contemporary Problems, 69, 7–46.
Battista, S. R., & Kocovski, N. L. (2010). Exploring the effect of alcohol on post-event processing specific to a social event. Cognitive Behaviour Therapy, 39, 1–10.
Baumeister, A. A., & Hawkins, M. F. (2004). The serotonin hypothesis of schizophrenia: A historical case study on the heuristic value of theory in clinical neuroscience. Journal of the History of the Neurosciences, 13, 277–291.
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York, NY: International Universities Press.
Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological correlates. American Journal of Psychiatry, 165, 969–977.
Beucke, J. C., Sepulcre, J., Talukdar, T., Linnman, C., Zschenderlein, K., Endrass, T., . . . Kathman, N. (2013). Abnormally high degree connectivity of the orbitofrontal cortex in obsessive-compulsive disorder. JAMA Psychiatry, 70, 619–629.
Biederman, J., Faraone, S. V., Hirshfeld-Becker, D. R., Friedman, D., Robin, J. A., & Rosenbaum, J. F. (2001). Patterns of psychopathology and dysfunction in high-risk children of parents with panic disorder and major depression. American Journal of Psychiatry, 158, 49–57.
Bolton, D., Rijsdijk, F., O’Connor, T. G., Perrin, S., & Eley, T. C. (2007). Obsessive-compulsive disorder, tics and anxiety in 6-year-old twins. Psychological Medicine, 37, 39–48.
Bourguignon, E. (1970). Hallucinations and trance: An anthropologist’s perspective. In W. Keup (Ed.), Origins and mechanisms of hallucination (pp. 183–190). New York, NY: Plenum Press.
Bouton, M. E., Mineka, S., & Barlow, D. H. (2001). A modern learning theory perspective on the etiology of panic disorder. Psychological Review, 108, 4–32.
Brewin, C. R., Andrews, B., & Valentine, J. D. (2000). Meta-analysis of risk factors for posttraumatic stress disorder in trauma-exposed adults. Journal of Consulting and Clinical Psychology, 68, 748–756.
Bremner, J. D., Krystal, J. H., Southwick, S. M., & Charney, D. S. (1996). Noradrenergic mechanisms in stress and anxiety: I. preclinical studies. Synapse, 23, 28–38.
Brown, A. S., Begg, M. D., Gravenstein, S., Schaefer, C. A., Wyatt, R. J., Breshnahan, M., . . . Susser, E. S. (2004). Serologic evidence of prenatal influenza in the etiology of schizophrenia. Archives of General Psychiatry, 61, 774–780.
Boland, R. J., & Keller, M. B. (2009). Course and outcome of depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 23–43). New York, NY: Guilford Press.
Brown, G. W., & Harris, T. O. (1989). Depression. In G. W. Brown and T. O. Harris (Eds.), Life events and illness (pp. 49–93). New York, NY: Guilford Press.
Brown, G. W., Ban, M., Craig, T. J. K., Harris, T. O., Herbert, J., & Uher, R. (2013). Serotonin transporter length polymorphism, childhood maltreatment, and chronic depression: A specific gene-environment interaction. Depression and Anxiety, 30, 5–13.
Buchsbaum, M. S., Nuechterlein, K. H., Haier, R. J., Wu, J., Sicotte, N., Hazlett, E., . . . Guich, S. (1990). Glucose metabolic rate in normal and schizophrenics during the continuous performance test assessed by positron emission tomography. British Journal of Psychiatry, 156, 216–227.
Butler, L. D., & Nolen-Hoeksema, S. (1994). Gender differences in responses to depressed mood in a college sample. Sex Roles, 30, 331–346.
Cannon, M., Jones, P. B., & Murray, R. M. (2002). Obstetric complications and schizophrenia: Historical and meta-analytic review. American Journal of Psychiatry, 159, 1080–1092.
Casadio, P., Fernandes, C., Murray, R. M., & Di Forti, M. (2011). Cannabis use in young people: The risk for schizophrenia. Neuroscience and Biobehavioral Reviews, 35, 1779–1787.
Cardeña, E., & Gleaves, D. H. (2006). Dissociative disorders. In M. Hersen, S. M. Turner, & D. C. Beidel (Eds.), Adult psychopathology and diagnosis (pp. 473–503). Hoboken, NJ: John Wiley & Sons.
Caspi, A., Sugden, K., Moffitt, T. E., Taylor, A., Craig, I. W., Harrington, H., Poulton, R. (2003). Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science, 301(5631), 386–389.
Charney, D. S., Woods, S. W., Nagy, L. M., Southwick, S. M., Krystal, J. H., & Heninger, G. R. (1990). Noradrenergic function in panic disorder [Supplemental material]. Journal of Clinical Psychiatry, 51, 5–11.
Clark, D. M. (1996). Panic disorder: From theory to therapy. In R. M. Rapee (Ed.), Current controversies in the anxiety disorders (pp. 318–344). New York, NY: Guilford Press.
Clauss, J. A., & Blackford, J. U. (2012). Behavioral inhibition and risk for developing social anxiety disorder: A meta-analytic study. Journal of the American Academy of Child and Adolescent Psychiatry, 51(10), 1066–1075.
Clegg, J. W. (2012). Teaching about mental health and illness through the history of the DSM. History of Psychology, 15, 364–370.
Cook, M., & Mineka, S. (1989). Observational conditioning of fear to fear-relevant versus fear-irrelevant stimuli in rhesus monkeys. Journal of Abnormal Psychology, 98, 448–459.
Craske, M. G. (1999). Anxiety disorders: Psychological approaches to theory and treatment. Boulder, CO: Westview Press.
Dalenberg, C. J., Brand, B. L., Gleaves, D. H., Dorahy, M. J., Loewenstein, R. J., Cardeña, E., . . . Spiegel, D. (2012). Evaluation of the evidence for the trauma and fantasy models of dissociation. Psychological Bulletin, 138, 550–588.
Davidson, R. J., Pizzagalli, D. A., & Nitschke, J. B. (2009). Representation and regulation of emotional depression: Perspectives from cognitive neuroscience. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 218–248). New York, NY: Guilford Press.
Davis, K. L., Kahn, R. S., Ko., G., & Davidson, M. (1991). Dopamine in schizophrenia: A review and reconceptualization. American Journal of Psychiatry, 148, 1474–1486.
Demos, J. (1983). Entertaining Satan: Witchcraft and the culture of early New England. New York, NY: Oxford University Press.
DiGrande, L., Perrin, M. A., Thorpe, L. E., Thalji, L., Murphy, J., Wu, D., . . . Brackbill, R. M. (2008). Posttraumatic stress symptoms, PTSD, and risk factors among lower Manhattan residents 2–3 years after the September 11, 2001 terrorist attacks. Journal of Traumatic Stress, 21, 264–273.
Dozois, D. J. A., & Beck, A. T. (2008). Cognitive schemas, beliefs and assumptions. In K. S. Dobson & D. J. A. Dozois (Eds.), Risk factors in depression (pp. 121–143). New York, NY: Academic Press.
Drevets, W. C., Bogers, W. U., & Raichle, M. E. (2002). Functional anatomical correlates of antidepressant drug treatment assessed using PET measures of regional glucose metabolism. European Neuropsychopharmacology, 12, 527–544.
Ehlers, A., & Clark, D. M. (2000). A cognitive model of posttraumatic stress disorder. Behaviour Research and Therapy, 38, 319–345.
Fields, T. (2010). Postpartum depression effects on early interactions, parenting, and safety practices: A review. Infant Behavior and Development, 33, 1–6.
Fisher, C. (2010, February 11). DSM-5 development process included emphasis on gender and cultural sensitivity [Web log post]. Retrieved from http://www.bmedreport.com/archives/9359
Fitzgerald, P. B., Laird, A. R., Maller, J., & Daskalakis, Z. J. (2008). A meta-analytic study of changes in brain activation in depression. Human Brain Mapping, 29, 683–695.
Foote, B., Smolin, Y., Kaplan, M., Legatt, M. E., & Lipschitz, D. (2006). Prevalence of dissociative disorders in psychiatric outpatients. American Journal of Psychiatry, 163, 623–629.
Fox, N. A., Henderson, H. A., Marshall, P. J., Nichols, K. E., & Ghera, M. M. (2005). Behavioral inhibition: Linking biology and behavior within a developmental framework. Annual Review of Psychology, 56, 235–262.
Frances, A. (2012, December 2). DSM 5 is guide not bible—ignore its ten worst changes [Web log post]. Retrieved from http://www.psychologytoday.com/blog/dsm5-in-distress/201212/dsm-5-is-guide-not-bible-ignore-its-ten-worst-changes
Fusar-Poli, P., Borgwardt, S., Bechdolf, A., Addington, J., Riecher-Rössler, A., Schultze-Lutter, F., . . . Yung, A. (2013). The psychosis high-risk state: A comprehensive state-of-the-art review. Archives of General Psychiatry, 70, 107–120.
Goldstein, A. J., & Chambless, D. L. (1978). A reanalysis of agoraphobia. Behavior Therapy, 9, 47–59.
Goldstein, J. M., Buka, S. L., Seidman, L. J., & Tsuang, M. T. (2010). Specificity of familial transmission of schizophrenia psychosis spectrum and affective psychoses in the New England family study’s high-risk design. Archives of General Psychiatry, 67, 458–467.
Good, B. J., & Hinton, D. E. (2009). Panic disorder in cross-cultural and historical perspective. In D. E. Hinton & B. J. Good (Eds.), Culture and panic disorder (pp. 1–28). Stanford, CA: Stanford University Press.
Goodman, S. H., & Brand, S. R. (2009). Depression and early adverse experiences. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 249–274). New York, NY: Guilford Press.
Gotlib, I. H., & Joormann, J. (2010). Cognition and depression: Current status and future directions. Annual Review of Clinical Psychology, 6, 285–312.
Gottesman, I. I. (2001). Psychopathology through a life span-genetic prism. American Psychologist, 56, 867–878.
Graybiel, A. N., & Rauch, S. L. (2000). Toward a neurobiology of obsessive-compulsive disorder. Neuron, 28, 343–347.
Green, M. F. (2001). Schizophrenia revealed: From neurons to social interactions. New York, NY: W. W. Norton.
Hackmann, A., Clark, D. M., & McManus, F. (2000). Recurrent images and early memories in social phobia. Behaviour Research and Therapy, 38, 601–610.
Halligan, S. L., Herbert, J., Goodyer, I., & Murray, L. (2007). Disturbances in morning cortisol secretion in association with maternal postnatal depression predict subsequent depressive symptomatology in adolescents. Biological Psychiatry, 62, 40–46.
Hasin, D. S., Fenton, M. C., & Weissman, M. M. (2011). Epidemiology of depressive disorders. In M. T. Tsuang, M. Tohen, & P. Jones (Eds.), Textbook of psychiatric epidemiology (pp. 289–309). Hoboken, NJ: John Wiley & Sons.
Herman, J. (1997). Trauma and recovery: The aftermath of violence—from domestic abuse to political terror. New York, NY: Basic Books.
Heston, L. L. (1966). Psychiatric disorders in foster home reared children of schizophrenic mothers. British Journal of Psychiatry, 112, 819–825.
Hettema, J. M., Neale, M. C., & Kendler, K. S. (2001). A review and meta-analysis of the genetic epidemiology of anxiety disorders. The American Journal of Psychiatry, 158, 1568–1578.
Holsboer, F., & Ising, M. (2010). Stress hormone regulation: Biological role and translation into therapy. Annual Review of Psychology, 61, 81–109.
Howes, O. D., & Kapur, S. (2009). The dopamine hypothesis of schizophrenia: Version III—The final common pathway. Schizophrenia Bulletin, 35, 549–562.
Johnson, J. G., Cohen, P., Kasen, S., & Brook, J. S. (2006). Dissociative disorders among adults in the community, impaired functioning, and axis I and II comorbidity. Journal of Psychiatric Research, 40, 131–140.
Joormann, J. (2009). Cognitive aspects of depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 298–321). New York, NY: Guilford Press.
Judd, L. L. (2012). Dimensional paradigm of the long-term course of unipolar major depressive disorder. Depression and Anxiety, 29, 167–171.
Kagan, J., Reznick, J. S., & Snidman, N. (1988). Biological bases of childhood shyness. Science, 240, 167–171.
Katzelnick, D. J., Kobak, K. A., DeLeire, T., Henk, H. J., Greist, J. H., Davidson, J. R. T., . . . Helstad, C. P. (2001). Impact of generalized social anxiety disorder in managed care. The American Journal of Psychiatry, 158, 1999–2007.
Kendler, K. S., Hettema, J. M., Butera, F., Gardner, C. O., & Prescott, C. A. (2003). Life event dimensions of loss, humiliation, entrapment, and danger in the prediction of onsets of major depression and generalized anxiety. Archives of General Psychiatry, 60, 789–796.
Kessler, R. C. (1997). The effects of stressful life events on depression. Annual Review of Psychology, 48, 191–214.
Kessler, R. C. (2003). Epidemiology of women and depression. Journal of Affective Disorders, 74, 5–13.
Kessler, R. C., Chiu, W. T., Jin, R., Ruscio, A. M., Shear, K., & Walters, E. (2006). The epidemiology of panic attacks, panic disorder, and agoraphobia in the National Comorbidity Survey Replication. Archives of General Psychiatry, 63, 415–424.
Kessler, R. C., Galea, S., Gruber, M. J., Sampson, N. A., Ursano, R. J., & Wessely, S. (2008). Trends in mental illness and suicidality after Hurricane Katrina. Molecular Psychiatry, 13, 374–384.
Kessler, R. C., Ruscio, A. M., Shear, K., & Wittchen, H. U. (2009). Epidemiology of anxiety disorders. In M. B. Stein & T. Steckler (Eds.), Behavioral neurobiology of anxiety and its treatment (pp. 21–35). New York, NY: Springer.
Kessler, R. C. Sonnega, A., Bromet, E., Hughes, M., & Nelson, C. B. (1995). Posttraumatic stress disorder in the National Comorbidity Survey. Archives of General Psychiatry, 52, 1048–1060.
Kessler, R. C., & Wang, P. S. (2009). Epidemiology of depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 5–22). New York, NY: Guilford Press.
Khashan, A. S., Abel, K. M., McNamee, R., Pedersen, M. G., Webb, R., Baker, P., . . . Mortensen, P. B. (2008). Higher risk of offspring schizophrenia following antenatal maternal exposure to severe adverse life events. Archives of General Psychiatry, 65, 146–152.
Kleim, B., Gonzalo, D., & Ehlers, A. (2011). The Depressive Attributions Questionnaire (DAQ): Development of a short self-report measure of depressogenic attributions. Journal of Psychopathology and Behavioral Assessment, 33, 375–385.
Koenen, K. C., Stellman, J. M., Stellman, S. D., & Sommer, J. F. (2003). Risk factors for course of posttraumatic stress disorder among Vietnam veterans: A 14-year follow-up of American Legionnaires. Journal of Consulting and Clinical Psychology, 71, 980–986.
Kopell, B. H., & Greenberg, B. D. (2008). Anatomy and physiology of the basal ganglia: Implications for DBS in psychiatry. Neuroscience and Biobehavioral Reviews, 32, 408–422.
Large, M., Sharma, S., Compton, M. T., Slade, T., & Nielssen, O. (2011). Cannabis use and earlier onset of psychosis: A systematic meta-analysis. Archives of General Psychiatry, 68, 555–561.
Lasalvia, A., Zoppei, S., Van Bortel, T., Bonetto, C., Cristofalo, D., Wahlbeck, K., Thornicroft, G. (2013). Global pattern of experienced and anticipated discrimination reported by people with major depressive disorder: A cross-sectional survey. The Lancet, 381, 55–62.
Lawrie, S. M., & Abukmeil, S. S. (1998). Brain abnormality in schizophrenia: A systematic and quantitative review of volumetric magnetic resonance imaging studies. British Journal of Psychiatry, 172, 110–120.
LeMoult, J., Castonguay, L. G., Joormann, J., & McAleavey, A. (2013). Depression. In L. G. Castonguay & T. F. Oltmanns (Eds.), Psychopathology: From science to clinical practice (pp. 17–61). New York, NY: Guilford Press.
Lilienfeld, S. O., & Marino, L. (1999). Essentialism revisited: Evolutionary theory and the concept of mental disorder. Journal of Abnormal Psychology, 108, 400–411.
Mackin, P., & Young, A. H. (2004, May 1). The role of cortisol and depression: Exploring new opportunities for treatments. Psychiatric Times. Retrieved from http://www.psychiatrictimes.com/articles/role-cortisol-and-depression-exploring-new-opportunities-treatments
Maher, W. B., & Maher, B. A. (1985). Psychopathology: I. from ancient times to the eighteenth century. In G. A. Kimble & K. Schlesinger (Eds.), Topics in the history of psychology: Volume 2 (pp. 251–294). Hillsdale, NJ: Erlbaum.
Marker, C. D. (2013, March 3). Safety behaviors in social anxiety: Playing it safe in social anxiety [Web log post]. Retrieved from http://www.psychologytoday.com/blog/face-your-fear/201303/safety-behaviors-in-social-anxiety
Martens, E. J., de Jonge, P., Na, B., Cohen, B. E., Lett, H., & Whooley, M. A. (2010). Scared to death? Generalized anxiety disorder and cardiovascular events in patients with stable coronary heart disease. Archives of General Psychiatry, 67, 750–758.
Mataix-Cols, D., Frost, R. O., Pertusa, A., Clark, L. A., Saxena, S., Leckman, J. F., . . . Wilhelm, S. (2010). Hoarding disorder: A new diagnosis for DSM-V? Depression and Anxiety, 27, 556–572.
Mayes, R., & Horowitz, A. V. (2005). DSM-III and the revolution in the classification of mental illness. Journal of the History of the Behavioral Sciences, 41, 249–267.
Mazure, C. M. (1998). Life stressors as risk factors in depression. Clinical Psychology: Science and Practice, 5, 291–313.
McCabe, R. E., Antony, M. M., Summerfeldt, L. J., Liss, A., & Swinson, R. P. (2003). Preliminary examination of the relationship between anxiety disorders in adults and self-reported history of teasing or bullying experiences. Cognitive Behaviour Therapy, 32, 187–193.
McEwen, B. S. (2005). Glucocorticoids, depression, and mood disorders: Structural remodeling in the brain. Metabolism: Clinical and Experimental, 54, 20–23.
McNally, R. J. (2003). Remembering trauma. Cambridge, MA: Harvard University Press.
Merikangas, K. R., & Tohen, M. (2011). Epidemiology of bipolar disorder in adults and children. In M. T. Tsuang, M. Tohen, & P. Jones (Eds.), Textbook of psychiatric epidemiology (pp. 329–342). Hoboken, NJ: John Wiley & Sons.
Merikangas, K. R., Jin, R., He, J. P., Kessler, R. C., Lee, S., Sampson, N. A., Zarkov, Z. (2011). Prevalence and correlates of bipolar spectrum disorder in the World Mental Health Survey Initiative. Archives of General Psychiatry, 68, 241–251.
Mezzich, J. E. (2002). International surveys on the use of ICD-10 and related diagnostic systems. Psychopathology, 35, 72–75.
Michaud, K., Matheson, K., Kelly, O., & Anisman, H. (2008). Impact of stressors in a natural context on release of cortisol in healthy adult humans: A meta-analysis. Stress, 11, 177–197.
Mineka, S., & Cook, M. (1993). Mechanisms involved in the observational conditioning of fear. Journal of Experimental Psychology: General, 122, 23–38.
Moitra, E., Beard, C., Weisberg, R. B., & Keller, M. B. (2011). Occupational impairment and social anxiety disorder in a sample of primary care patients. Journal of Affective Disorders, 130, 209–212.
Moffitt, T. E., Caspi, A., Harrington, H., Milne, B. J., Melchior, M., Goldberg, D., & Poulton, R. (2007). Generalized anxiety disorder and depression: Childhood risk factors in a birth cohort followed to age 32. Psychological Medicine, 37, 441–452.
Moore, T. H., Zammit, S., Lingford-Hughes, A., Barnes, T. R., Jones, P. B., Burke, M., & Lewis, G. (2007). Cannabis use and risk of psychotic or affective mental health outcomes. Lancet, 370, 319–328.
Morris, E. P., Stewart, S. H., & Ham, L. S. (2005). The relationship between social anxiety disorder and alcohol use disorders: A critical review. Clinical Psychology Review, 25, 734–760.
Mowrer, O. H. (1960). Learning theory and behavior. New York, NY: John Wiley & Sons.
Nader, K. (2001). Treatment methods for childhood trauma. In J. P. Wilson, M. J. Friedman, & J. D. Lindy (Eds.), Treating psychological trauma and PTSD (pp. 278–334). New York, NY: Guilford Press.
Nanni, V., Uher, R., & Danese, A. (2012). Childhood maltreatment predicts unfavorable course of illness and treatment outcome in depression: A meta-analysis. American Journal of Psychiatry, 169, 141–151.
National Comorbidity Survey. (2007). NCS-R lifetime prevalence estimates [Data file]. Retrieved from http://www.hcp.med.harvard.edu/ncs/index.php
National Institute on Drug Abuse (NIDA). (2007, October). Comorbid drug use and mental illness: A research update from the National Institute on Drug Abuse. Retrieved from http://www.drugabuse.gov/sites/default/files/comorbid.pdf
Nestadt, G., Samuels, J., Riddle, M., Bienvenu, J., Liang, K. Y., LaBuda, M., . . . Hoehn-Saric, R. (2000). A family study of obsessive-compulsive disorder. Archives of General Psychiatry, 57, 358–363.
Newman, C. F. (2004). Suicidality. In S. L. Johnson & R. L. Leahy (Eds.), Psychological treatment of bipolar disorder (pp. 265–285). New York, NY: Guilford Press.
Nolen-Hoeksema, S. (1987). Sex differences in unipolar depression: Evidence and theory. Psychological Bulletin, 101, 259–282.
Nolen-Hoeksema, S. (1991). Responses to depression and their effects on the duration of depressive episodes. Journal of Abnormal Psychology, 100, 569–582.
Nolen-Hoeksema, S. & Hilt, L. M. (2009). Gender differences in depression. In I. H. Gotlib & C. L. Hammen (Eds.), Handbook of depression (pp. 386–404). New York, NY: Guilford Press.
Norberg, M. M., Calamari, J. E., Cohen, R. J., & Riemann, B. C. (2008). Quality of life in obsessive-compulsive disorder: An evaluation of impairment and a preliminary analysis of the ameliorating effects of treatment. Depression and Anxiety, 25, 248–259.
Novick, D. M., Swartz, H. A., & Frank, E. (2010). Suicide attempts in bipolar I and bipolar II disorder: A review and meta-analysis of the evidence. Bipolar Disorders, 12, 1–9.
Noyes, R. (2001). Comorbidity in generalized anxiety disorder. Psychiatric Clinics of North America, 24, 41–55.
Öhman, A., & Mineka, S. (2001). Fears, phobias, and preparedness: Toward an evolved module of fear and fear learning. Psychological Review, 108, 483–552.
Olsson, A., & Phelps, E. A. (2007). Social learning of fear. Nature Neuroscience, 10, 1095–1102.
Oltmanns, T. F., & Castonguay, L. G. (2013). General issues in understanding and treating psychopathology. In L. G. Castonguay & T. F. Oltmanns (Eds.), Psychopathology: From science to clinical practice (pp. 1–16). New York, NY: Guilford Press.
Orr, S. P., Metzger, L. J., Lasko, N. B., Macklin, M. L., Peri, T., & Pitman, R. K. (2000). De novo conditioning in trauma-exposed individuals with and without posttraumatic stress disorder. Journal of Abnormal Psychology, 109, 290–298.
Ozer, E. J., Best, S. R., Lipsey, T. L., & Weiss, D. S. (2003). Predictors of posttraumatic stress disorder and symptoms in adults: A meta-analysis. Psychological Bulletin, 129, 52–73.
Patterson, M. L., Iizuka, Y., Tubbs, M. E., Ansel, J., Tsutsumi, M., & Anson, J. (2007). Passing encounters east and west: Comparing Japanese and American pedestrian interactions. Journal of Nonverbal Behavior, 31, 155–166.
Pauls, D. L. (2010). The genetics of obsessive-compulsive disorder: A review. Dialogues in Clinical Neuroscience, 12, 149–163.
Paykel, E. S. (2003). Life events and affective disorders [Supplemental material]. Acta Psychiatrica Scandinavica, 108(S418), 61–66.
Pazain, M. (2010, December 2). To look or not to look? Eye contact differences in different cultures [Web log post]. Retrieved from http://www.examiner.com/article/to-look-or-not-to-look-eye-contact-differences-different-cultures
Phan, K. L., Fitzgerald, D. A., Nathan, P. J., Moore, G. J., Uhde, T. W., & Tancer, M. E. (2005). Neural substrates for voluntary suppression of negative affect: A functional magnetic resonance imaging study. Biological Psychiatry, 57, 210–219.
Phillips, K. (2005). The broken mirror: Understanding and treating body dysmorphic disorder. Oxford, England: Oxford University Press.
Piper, A., & Merskey, H. (2004). The persistence of folly: A critical examination of dissociative identity disorder: Part I: The excesses of an improbable concept. Canadian Journal of Psychiatry, 49, 592–600.
Pittman, R. K. (1988). Post-traumatic stress disorder, conditioning, and network theory. Psychiatric Annals, 18, 182–189.
Pope, H. G., Jr., Barry, S. B., Bodkin, A., & Hudson, J. I. (2006). Tracking scientific interest in the dissociative disorders: A study of scientific publication output 1984–2003. Psychotherapy and Psychosomatics, 75, 19–24.
Pope, H. G., Jr., Hudson, J. I., Bodkin, J. A., & Oliva, P. S. (1998). Questionable validity of ‘dissociative amnesia’ in trauma victims: Evidence from prospective studies. British Journal of Psychiatry, 172, 210–215.
Pope, H. G., Jr., Poliakoff, M. B., Parker, M. P., Boynes, M., & Hudson, J. I. (2006). Is dissociative amnesia a culture-bound syndrome? Findings from a survey of historical literature. Psychological Medicine, 37, 225–233.
Putnam, F.W., Guroff, J, J., Silberman, E. K., Barban, L., & Post, R. M. (1986). The clinical phenomenology of multiple personality disorder: A review of 100 recent cases. Journal of Clinical Psychiatry, 47, 285–293.
Rachman, S. (1977). The conditioning theory of fear acquisition: A critical examination. Behaviour Theory and Research, 15, 375–387.
Regier, D. A., Kuhl, E. A., & Kupfer, D. A. (2012). DSM-5: Classification and criteria changes. World Psychiatry, 12, 92–98.
Robinson, M. S., & Alloy, L. B. (2003). Negative cognitive styles and stress-reactive rumination interact to predict depression: A prospective study. Cognitive Therapy and Research, 27, 275–292.
Roche, T. (2002, March 18). Andrea Yates: More to the story. Time. Retrieved from http://content.time.com/time/nation/article/0,8599,218445,00.html.
Root, B. A. (2000). Understanding panic and other anxiety disorders. Jackson, MS: University Press of Mississippi.
Ross, C. A., Miller, S. D., Reagor, P., Bjornson, L., Fraser, G. A., & Anderson, G. (1990). Structured interview data on 102 cases of multiple personality disorder from four centers. The American Journal of Psychiatry, 147, 596–601.
Rothschild, A. J. (1999). Mood disorders. In A. M. Nicholi, Jr. (Ed.), The Harvard guide to psychiatry (pp. 281–307). Cambridge, MA: The Belknap Press of Harvard University.
Ruscio, A. M., Stein, D. J., Chiu, W. T., & Kessler, R. C. (2010). The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication. Molecular Psychiatry, 15, 53–63.
Rushworth, M. F., Noonan, M. P., Boorman, E. D., Walton, M. E., & Behrens, T. E. (2011). Frontal cortex and reward-guided learning and decision-making. Neuron, 70, 1054–1069.
Rotge, J. Y., Guehl, D., Dilharreguy, B., Cuny, E., Tignol, J., Biolac, B., . . . Aouizerate, B. (2008). Provocation of obsessive-compulsive symptoms: A quantitative voxel-based meta-analysis of functional neuroimaging studies. Journal of Psychiatry and Neuroscience, 33, 405–412.
Saxena, S., Bota, R. G., & Brody, A. L. (2001). Brain-behavior relationships in obsessive- compulsive disorder. Seminars in Clinical Neuropsychiatry, 6, 82–101.
Schwartz, T. (1981). The hillside strangler: A murderer’s mind. New York, NY: New American Library.
Seligman, M. E. P. (1971). Phobias and preparedness. Behavioral Therapy, 2, 307–320.
Shih, R. A., Belmonte, P. L., & Zandi, P. P. (2004). A review of the evidence from family, twin, and adoption studies for a genetic contribution to adult psychiatric disorders. International Review of Psychiatry, 16, 260–283.
Siegle, G. J., Thompson, W., Carter, C. S., Steinhauer, S. R., & Thase, M. E. (2007). Increased amygdala and decreased dorsolateral prefrontal BOLD responses in unipolar depression: Related and independent features. Biological Psychiatry, 61, 198–209.
Silverstein, C. (2009). The implications of removing homosexuality from the DSM as a mental disorder. Archives of Sexual Behavior, 38, 161–163.
Simon, D., Kaufmann, C., Müsch, K., Kischkel, E., & Kathmann, N. (2010). Fronto-striato-limbic hyperactivation in obsessive-compulsive disorder during individually tailored symptom provocation. Psychophysiology, 47(4), 728–738. doi:10.1111/j.1469-8986.2010.00980.x
Snyder, S. H. (1976). The dopamine hypothesis of schizophrenia: Focus on the dopamine receptor. The American Journal of Psychiatry, 133, 197–202.
Stein, M. B., & Kean, Y. M. (2000). Disability and quality of life in social phobia: Epidemiological findings. The American Journal of Psychiatry, 157, 1606–1613.
Steinmetz, J. E., Tracy, J. A., & Green, J. T. (2001). Classical eyeblink conditioning: Clinical models and applications.
Licenses and Attributions (Click to expand)
CC licensed content, Original
- Psychological disorders. Authored by Karenna Malavanti. Provided by Pressbooks. License: CC BY-NC-SA: Attribution-NonCommercial-ShareAlike
CC licensed content, Shared previously
- Why It Matters: Psychological Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY-SA: Attribution-ShareAlike Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/introduction-2/
- Psychological Disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-1-what-are-psychological-disorders.
- Homelessness and Mental Health. Provided by: Wikipedia. License: CC BY-SA: Attribution-ShareAlike. Located at: https://en.wikipedia.org/wiki/Homelessness_and_mental_health.
- Mental Illness Image. Authored by: Magnus Manske. Provided by: Wikipedia. License: CC BY: Attribution Located at: https://upload.wikimedia.org/wikipedia/commons/9/93/Mental_illness_%284199789866%29.jpg.
- Introduction to Psychological Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/introduction-to-psychological-disorders/
- What Are Psychological Disorders?. Authored by: OpenStax College.License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-1-what-are-psychological-disorders.
- Image of anguish. Authored by: Porsche Brosseau. License: CC BY: Attribution. Located at: https://www.flickr.com/photos/porsche-linn/5561412422.
- What are Psychological Disorders?. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/what-are-psychological-disorders/
- Diagnosing and Classifying Psychological Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/diagnosing-and-classifying-psychological-disorders/
- Diagnosing and Classifying Psychological Disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-2-diagnosing-and-classifying-psychological-disorders.
- Perspectives on Psychological Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/perspectives-on-psychological-disorders/
- Perspectives on Psychological Disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-3-perspectives-on-psychological-disorders.
- Introduction to Anxiety Disorders, OCD, and PTSD. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY-NC-SA: Attribution-NonCommercial-ShareAlike Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/introduction-to-anxiety-disorders-and-ocd/
- Learning objective. Provided by: Open Learning Initiative. License: CC BY-NC-SA: Attribution-NonCommercial-ShareAlike. Located at: https://oli.cmu.edu/jcourse/webui/syllabus/module.do?context=4c3948bb80020ca601248e443ee39040.
- Anxiety Disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-4-anxiety-disorders.
- Phobias and Social Anxiety Disorder. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY-NC-SA: Attribution-NonCommericalShareAlike Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/anxiety-disorders/.
- Tyre Agora. Authored by: Heretiq. License: CC BY-SA: Attribution-ShareAlike. Located at: https://en.wikipedia.org/wiki/Agora#/media/File:TyreAlMinaAgora.jpg.
- Agoraphobia. Provided by: Wikipedia. License: CC BY-SA: Attribution-ShareAlike. Located at: https://en.wikipedia.org/wiki/Agoraphobia.
- Anxious man image. Authored by: Bada Bing. Provided by: Flickr. License: CC BY-SA: Attribution-ShareAlike. Located at: https://www.flickr.com/photos/zetson/3241975525.
- Anxiety and Related Disorders caption for image. Authored by: David H. Barlow and Kristen K. Ellard . Provided by: Boston University, Massachusetts General Hospital, Harvard Medical School. License: CC BY-NC-SA: Attribution-NonCommercial-ShareAlike. Located at: http://nobaproject.com/modules/anxiety-and-related-disorders.
- Panic and Generalized Anxiety Disorder. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/social-anxiety-disorder-and-generalized-anxiety-disorder/
- Obsessive-Compulsive and Related Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/obsessive-compulsive-and-related-disorders/
- Obsessive-Compulsive and Related Disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-5-obsessive-compulsive-and-related-disorders.
- Posttraumatic Stress Disorder. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/posttraumatic-stress-disorder/
- Posttraumatic Stress Disorder. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-6-posttraumatic-stress-disorder.
- Introduction to Mood Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/introduction-to-mood-disorders/
- Mood Disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-7-mood-disorders.
- image of woman. Authored by: gratisography. Provided by: Pexels. License: CC0: No Rights Reserved. Located at: https://www.pexels.com/photo/black-and-white-woman-girl-sitting-2369/.
- Major Depressive Disorder. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/major-depressive-disorder/
- Bipolar Disorder. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/mood-disorders/
- The Biological Basis of Mood Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/the-biological-basis-of-mood-disorders/
- Introduction to Schizophrenia and Dissociative Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/introduction-to-schizophrenia-and-dissociative-disorders/
- Schizophrenia. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-8-schizophrenia.
- Dissociative disorders. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-9-dissociative-disorders.
- Word Salad. Authored by: CopperKettle. Provided by: Wikipedia. License: CC BY: Attribution. Located at: https://simple.wikipedia.org/wiki/Schizophrenia#/media/File:Artistic_view_of_how_the_world_feels_like_with_schizophrenia_-_journal.pmed.0020146.g001.jpg.
- Schizophrenia. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY-SA: Attribution-ShareAlike Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/schizophrenia/
- Information on positive symptoms of schizophrenia. Provided by: Boundless. Project: Boundless Psychology. License: CC BY-SA: Attribution-ShareAlike. Located at: https://www.boundless.com/psychology/textbooks/boundless-psychology-textbook/psychological-disorders-18/schizophrenia-spectrum-and-other-psychotic-disorders-94/introduction-to-schizophrenia-and-psychosis-360-12895/.
- Tactile hallucination image. Authored by: Angela Mariam Thomas. License: CC BY-SA: Attribution-ShareAlike. Located at: https://commons.wikimedia.org/wiki/File:Tactile_hallucination.jpg.
- Schizophrenia lobes picture. Authored by: BruceBlaus. License: CC BY-SA: Attribution-ShareAlike. Located at: https://commons.wikimedia.org/wiki/File:Schizophrenia_(Brain).png.
- Dissociative Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/dissociative-disorders/
- Review: Classifying Psychological Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY-SA: Attribution-ShareAlike Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/tutorial-mystery-client/
- Mental Disorders. Provided by: Wikipedia. License: CC BY-SA: Attribution-ShareAlike. Located at: https://en.wikipedia.org/wiki/Mental_disorder.
- Mystery Client interactive. Authored by: Jessica Traylor for Lumen Learning. Provided by: Lumen Learning. License: CC BY: Attribution
- Summaries from psychological disorders section. Authored by: OpenStax College. License: CC BY: Attribution. License Terms: Download for free at https://openstax.org/books/psychology-2e/pages/1-introduction. Located at: https://openstax.org/books/psychology-2e/pages/15-summary.
- play button icon. Authored by: kropekk_pl . License: CC0: No Rights Reserved. Located at: https://pixabay.com/en/icon-icons-button-buttons-theme-354294/.
- Disorders. Authored by: Lumen Learning Provided by: Lumen Learning. License: CC BY: Attribution Located at: https://pressbooks.online.ucf.edu/lumenpsychology/chapter/putting-it-together-psychological-disorders/
Public domain content
- Mental Health Myths. Provided by: U.S. Department of Health & Human Services. License: Public Domain: No Known Copyright. Located at: https://www.mentalhealth.gov/basics/mental-health-myths-facts.
- Recovery is Possible. Provided by: U.S. Department of Health & Human Services. License: Public Domain: No Known Copyright. Located at: https://www.mentalhealth.gov/basics/recovery-possible
- Battling PTSD image. Provided by: United States Marines. License: Public Domain: No Known Copyright. Located at: https://www.flickr.com/photos/marine_corps/4949341330.
- Photo of man. Authored by: David Ensor. License: Public Domain: No Known Copyright. Located at: https://www.flickr.com/photos/dbensor/5879429534.
All rights reserved content
- Psychological Disorders: Crash Course Psychology #28. Provided by: CrashCourse. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=wuhJ-GkRRQc&feature=youtu.be&list=PL8dPuuaLjXtOPRKzVLY0jJY-uHOH9KVU6.
- Debunking the myths of OCD. Authored by: Natascha M. Santos. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=DhlRgwdDc-E.
- OCD & Anxiety Disorders: Crash Course Psychology #29. Authored by: Hank Green. Provided by: CrashCourse. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=aX7jnVXXG5o&index=29&list=PL8dPuuaLjXtOPRKzVLY0jJY-uHOH9KVU6.
- Depressive and Bipolar Disorders: Crash Course Psychology #30. Authored by: Hank Green. Provided by: CrashCourse. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=ZwMlHkWKDwM&feature=youtu.be&list=PL8dPuuaLjXtOPRKzVLY0jJY-uHOH9KVU6.
- Schizophrenia & Dissociative Disorders: Crash Course Psychology #32. Authored by: Hank Green. Provided by: CrashCourse. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=uxktavpRdzU&feature=youtu.be&list=PL8dPuuaLjXtOPRKzVLY0jJY-uHOH9KVU6.
- #StigmaFree: Mayim Bialik. Authored by: NAMI. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=Gzk7sSOHGSQ.
- ARCHIATRIC. Authored by: Federico Babina. License: Other. License Terms: Standard YouTube License. Located at: https://www.youtube.com/watch?v=a3fTw-xzEM4.
characterized by excessive and persistent fear and anxiety, and by related disturbances in behavior
characterized by excessive and persistent fear and anxiety, and by related disturbances in behavior
emotions consist of two factors: physiological and cognitive
emotions arise from physiological arousal
lie detector test that measures physiological arousal of individuals as they answer a series of questions
lie detector test that measures physiological arousal of individuals as they answer a series of questions
emotions arise from physiological arousal
characterized by the tendency to experience intrusive and unwanted thoughts and urges (obsession) and/or the need to engage in repetitive behaviors or mental acts (compulsions) in response to the unwanted thoughts and urges
area of the frontal lobe involved in learning and decision-making
characterized by the tendency to experience intrusive and unwanted thoughts and urges (obsession) and/or the need to engage in repetitive behaviors or mental acts (compulsions) in response to the unwanted thoughts and urges
area of the frontal lobe involved in learning and decision-making
subjective state of being often described as feelings
subjective state of being often described as feelings
branch of psychology that studies the interactions between people working in organizations and the effects of those interactions on productivity
branch of psychology that studies job characteristics, applicant characteristics, and how to match them; also studies employee training and performance appraisal
branch of psychology that studies job characteristics, applicant characteristics, and how to match them; also studies employee training and performance appraisal
traits that employers cannot use to discriminate in hiring, benefits, promotions, or termination; these traits are fundamental to one’s personal identity (e.g. skin color and hair texture)
determining and listing tasks associated with a particular job
one of the culturally specific standards that govern the types and frequencies of emotions that are acceptable
branch of psychology that studies the interactions between people working in organizations and the effects of those interactions on productivity
one of the culturally specific standards that govern the types and frequencies of emotions that are acceptable
mental or behavioral efforts used to manage problems relating to stress, including its cause and the unpleasant feelings and emotions it produces
peoples’ beliefs concerning their capacity to influence and shape outcomes in their lives
one of a group of mood disorders in which depression is the defining feature
peoples’ beliefs concerning their capacity to influence and shape outcomes in their lives
evaluation of an employee’s success or lack of success at performing the duties of the job
evaluation of an employee’s success or lack of success at performing the duties of the job
requirement of certain occupations for which denying an individual employment would otherwise violate the law, such as requirements concerning religion or sex
scientific area of study seeking to identify and promote those qualities that lead to happy, fulfilled, and contented lives
area of the frontal lobe involved in learning and decision-making
employers cannot discriminate against any individual based on a disability
state or a trait that involves pleasurable engagement with the environment, the dimensions of which include happiness, joy, enthusiasm, alertness, and excitement
requirement of certain occupations for which denying an individual employment would otherwise violate the law, such as requirements concerning religion or sex
tendency toward a positive outlook and positive expectations
our emotions are determined by our appraisal of the stimulus
state involving intense engagement in an activity; usually is experienced when participating in creative, work, and leisure endeavors
state or a trait that involves pleasurable engagement with the environment, the dimensions of which include happiness, joy, enthusiasm, alertness, and excitement
traits that employers cannot use to discriminate in hiring, benefits, promotions, or termination; these traits are fundamental to one’s personal identity (e.g. skin color and hair texture)
employers cannot discriminate against any individual based on a disability
experiencing a profoundly traumatic event leads to a constellation of symptoms that include intrusive and distressing memories of the event, avoidance of stimuli connected to the event, negative emotional states, feelings of detachment from others, irritability, proneness toward outbursts, hypervigilance, and a tendency to startle easily; these symptoms must occur for at least one month
branch of psychology that studies how workers interact with the tools of work and how to design those tools to optimize workers’ productivity, safety, and health
branch of psychology that studies job characteristics, applicant characteristics, and how to match them; also studies employee training and performance appraisal
one of the culturally specific standards that govern the types and frequencies of emotions that are acceptable
facial expressions are capable of influencing our emotions
